
Valérie Chetboul
略語:ACRONYMS
•ACVIM American College of Veterinary Internal Medicine 米国獣医内科学会
•ALMS1 Alström syndrome protein 1 アルストローム症候群蛋白1
•ARVC arrhythmogenic right ventricular cardiomyopathy 不整脈原性右室心筋症
•ATE arterial thromboembolism 動脈血栓塞栓症
•CHF congestive heart failure うっ血性心不全
•DCM dilated cardiomyopathy 拡張型心筋症
•DLH Domestic Longhaired ドメスティック・ロングヘアー
•DSH Domestic Shorthaired ドメスティック・ショートヘアー
•ECG electrocardiographic 心電図学的
•HCM hypertrophic cardiomyopathy 肥大型心筋症
•IGF-1 insulin-like growth factor 1 インスリン様成長因子
•IV intravenous 静脈内
•IVS interventricular septum 心室中隔
•LA left atrial/atrium 左心房
•LAE left atrial enlargement 左心房拡大
•LOE levels of evidence エビデンスレベル
•LV left ventricle/ventricular 左心室/左室性
•LVH left ventricular hypertrophy 左室肥大
•LVOT left ventricular outflow tract 左室流出路
•LVOTO left ventricular outflow tract obstruction 左室流出路閉塞
•MV mitral valve 僧帽弁
•NSCM nonspecific cardiomyopathy 非特異的心筋症•ACVIM American College of Veterinary Internal Medicine 米国獣医内科学会
•ALMS1 Alström syndrome protein 1 アルストローム症候群蛋白1
•ARVC arrhythmogenic right ventricular cardiomyopathy 不整脈原性右室心筋症
•ATE arterial thromboembolism 動脈血栓塞栓症
•CHF congestive heart failure うっ血性心不全
•DCM dilated cardiomyopathy 拡張型心筋症
•DLH Domestic Longhaired ドメスティック・ロングヘアー
•DSH Domestic Shorthaired ドメスティック・ショートヘアー
•ECG electrocardiographic 心電図学的
•HCM hypertrophic cardiomyopathy 肥大型心筋症
•IGF-1 insulin-like growth factor 1 インスリン様成長因子
•IV intravenous 静脈内
•IVS interventricular septum 心室中隔
•LA left atrial/atrium 左心房
•LAE left atrial enlargement 左心房拡大
•LOE levels of evidence エビデンスレベル
•LV left ventricle/ventricular 左心室/左室性
•LVH left ventricular hypertrophy 左室肥大
•LVOT left ventricular outflow tract 左室流出路
•LVOTO left ventricular outflow tract obstruction 左室流出路閉塞
•MV mitral valve 僧帽弁
•NSCM nonspecific cardiomyopathy 非特異的心筋症
•NT-proBNP N-terminal pro-B-type natriuretic peptide N末端プロB型ナトリウム利尿ペプチド
•OHCM obstructive hypertrophic cardiomyopathy 閉塞性肥大型心筋症
•RCM restrictive cardiomyopathy 拘束型心筋症
•RV right ventricle/ventricular 右心室/右室性
•TDI tissue Doppler imaging 組織ドプラ法
•TV tricuspid valve 三尖弁
•VHS vertebral heart score 椎体心サイズ
•WHO World Health Organization 世界保健機関INTRODUCTION: CLASSIFICATION AND GENERAL PREVALENCE:緒論:分類および一般的有病率
CLASSIFICATION: HISTORICAL AND NOSOLOGICAL CONSIDERATIONS:分類:歴史的および疾病分類学的考察
Myocardial diseases refer to a broad spectrum of heterogeneous diseases of the heart muscle with variable phenotype and prognosis, and are by far the most common cardiac disorders in the cat.¹⁻⁵ Over the last 4 decades, several classifications of human myocardial diseases have been successively proposed and modified, due to the greatly increased knowledge of their various underlying causes, molecular genetic basis and complex pathophysiological features, as well as the discovery of new pathological entities.⁶⁻¹⁴ In 1980, the World Health Organization (WHO) identified “heart muscle diseases of unknown cause” as cardiomyopathies, which were differentiated from specific heart muscle diseases (of known cause).⁶ In 1995, the next WHO classification redefined cardiomyopathies as “diseases of myocardium associated with cardiac dysfunction” and added two newly recognized myocardial diseases to the list,⁷ i.e., arrhythmogenic right ventricular cardiomyopathy (ARVC) and restrictive cardiomyopathy (RCM), both described several years later in the cat.¹⁵⁻¹⁷ Cardiomyopathies were thus classified into 5 groups according to their dominant pathophysiologic mechanism, i.e., dilated cardiomyopathy (DCM), hypertrophic cardiomyopathy (HCM), RCM, ARVC, and unclassified cardiomyopathies, the latter including cases that did not fit into the 4 other phenotypes.⁷ An additional group named “specific cardiomyopathies” was also recognized, including myocardial diseases associated with specific cardiac or systemic disorders (e.g., ischemic, valvular, hypertensive, inflammatory, metabolic, toxic cardiomyopathies, and myocardial disorders associated with neuromuscular or general system diseases). In 2006, an expert committee of the American Heart Association proposed a new classification of cardiomyopathies with 2 major groups (primary vs. secondary) based on predominant organ involvement: primary cardiomyopathies (genetic, non-genetic, or mixed) were those solely or predominantly confined to the myocardium, whereas secondary cardiomyopathies showed myocardial involvement as part of numerous generalized systemic or multiorgan disorders.⁸ In 2008, the European Society of Cardiology (ESC) Working Group on Myocardial and Pericardial Diseases defined a cardiomyopathy as “a myocardial disorder in which the heart muscle is structurally and functionally abnormal, in the absence of coronary artery disease, hypertension, valvular disease and congenital heart disease sufficient to cause the observed myocardial abnormality.”¹¹ The ESC Working Group also proposed an updated classification of cardiomyopathies mainly based on the 5 phenotypes of the 1995 WHO classification (i.e., HCM, DCM, ARVC, RCM and unclassified phenotypes), and each myocardial phenotype was then subdivided into familial/genetic and non-familial/non-genetic forms.¹¹ However, all classification systems present limitations and the nosological approach to myocardial diseases still remains debated,¹⁸˒¹⁹ as a given etiology may be associated with a spectrum of myocardial phenotypes. Further, morphological and functional phenotypes can overlap and even evolve over time, while our etiological understanding of previously named idiopathic cardiomyopathies continues to improve.
心筋疾患とは、多様な表現型および予後を示す心筋の異質性疾患群を指し、猫において最も一般的な心疾患である。¹⁻⁵ 過去40年間にわたり、ヒトの心筋疾患に対する複数の分類体系が順次提唱・改訂されてきたが、その背景には、さまざまな基礎病因、分子遺伝学的基盤、複雑な病態生理学的特徴に関する知識の飛躍的増加、および新たな病理学的病態の発見がある。⁶⁻¹⁴1980年、世界保健機関(WHO)は「原因不明の心筋疾患」を心筋症として定義し、既知の原因を有する特異的心筋疾患と区別した。⁶ 1995年のWHO分類では、心筋症は「心機能障害を伴う心筋疾患」と再定義され、さらに新たに認識された2つの心筋疾患、すなわち不整脈原性右室心筋症(ARVC)および拘束型心筋症(RCM)が分類に追加された。⁷ これらはいずれも、その数年後に猫でも報告されている。¹⁵⁻¹⁷その結果、心筋症は主たる病態生理学的機序に基づき、拡張型心筋症(DCM)、肥大型心筋症(HCM)、RCM、ARVC、および未分類心筋症の5群に分類された。未分類心筋症には、他の4表現型のいずれにも該当しない症例が含まれた。⁷ また、「特異的心筋症」という追加群も認識され、虚血性、弁膜性、高血圧性、炎症性、代謝性、中毒性心筋症や、神経筋疾患あるいは全身性疾患に関連する心筋障害など、特定の心疾患または全身性疾患に関連した心筋疾患が含まれた。2006年には、米国心臓協会の専門委員会が、主たる臓器障害に基づき、心筋症を一次性と二次性の2大群に分類する新たな分類体系を提唱した。一次性心筋症(遺伝性、非遺伝性、混合型)は、心筋にのみ、あるいは主として心筋に限局する疾患であり、二次性心筋症は、全身性または多臓器疾患の一部として心筋病変を示すものとされた。⁸2008年には、欧州心臓病学会(ESC)の心筋・心膜疾患ワーキンググループが、心筋症を「観察される心筋異常を説明しうるほどの冠動脈疾患、高血圧、弁膜疾患、先天性心疾患が存在しないにもかかわらず、心筋が構造的および機能的に異常を呈する心筋障害」と定義した。¹¹ESCワーキンググループはまた、1995年WHO分類における5つの表現型(HCM、DCM、ARVC、RCM、および未分類表現型)を基盤とした更新分類を提唱し、各心筋表現型を家族性/遺伝性型と非家族性/非遺伝性型に細分類した。¹¹しかし、いずれの分類体系にも限界が存在し、心筋疾患に対する疾病分類学的アプローチについてはいまだ議論が続いている。¹⁸˒¹⁹ その理由として、同一病因が複数の心筋表現型と関連する可能性があること、さらに形態学的および機能的表現型が重複し、時間経過とともに変化しうることが挙げられる。また、従来「特発性」とされていた心筋症についても、その病因論的理解は現在も進歩し続けている。
AMERICAN COLLEGE OF VETERINARY INTERNAL MEDICINE (ACVIM) CONSENSUS STATEMENT ON FELINE CARDIOMYOPATHIES:猫の心筋症に関する米国獣医内科学会(ACVIM)コンセンサスステートメント
The 2020 report by the American College of Veterinary Internal Medicine (ACVIM) Consensus Statement panel on cardiomyopathies in cats proposed a simplified adaptation of the ESC definition and classification for use in cats.³˒¹¹ The ACVIM Consensus Statement thus defined cardiomyopathy as “a myocardial disorder in which the heart muscle is structurally and functionally abnormal in the absence of any other cardiovascular disease sufficient to cause the observed myocardial abnormality” and proposed a classification scheme based on phenotypic features, meaning structural and functional myocardial alterations (Table 234.1, Figure 234.1). This classification includes five cardiomyopathy phenotypes diagnosed by echocardiography, i.e., the HCM, RCM, DCM, and ARVC phenotypes, and the “nonspecific cardiomyopathy (NSCM) phenotype,” corresponding to the above-mentioned “unclassified phenotype.”³ If a cardiomyopathy phenotype is detected by echocardiography in a given cat (e.g., HCM phenotype), as long as its potential causes are sought (e.g., systemic hypertension, hyperthyroidism, myocarditis, neoplastic infiltration), the cat is said to have an “HCM phenotype.” If no underlying cause is found, the cat is then said to have HCM.³ This chapter on feline myocardial diseases will refer to this ACVIM classification system. Additionally, to be clearer for the reader and as proposed by the American Heart Association,⁸ primary cardiomyopathies will here refer to cardiomyopathies of unknown causes and secondary cardiomyopathies to cardiomyopathies of systemic origins or with specific etiologic factors.
2020年に発表された米国獣医内科学会(ACVIM)の猫の心筋症コンセンサスステートメントでは、ESCの定義および分類を猫用に簡略化した適応分類が提案された。³˒¹¹このACVIMコンセンサスステートメントでは、心筋症を「観察される心筋異常を説明しうる他の心血管疾患が存在しない状況下において、心筋が構造的および機能的に異常を呈する心筋障害」と定義し、構造的・機能的心筋変化、すなわち表現型的特徴に基づく分類体系を提唱した(表234.1、図234.1)。この分類には、心エコー検査により診断される5つの心筋症表現型、すなわちHCM、RCM、DCM、ARVC表現型、および前述の「未分類表現型」に対応する「非特異的心筋症(NSCM)表現型」が含まれる。³ある猫で心エコー検査により心筋症表現型(例えばHCM表現型)が認められた場合、その潜在的原因(全身性高血圧、甲状腺機能亢進症、心筋炎、腫瘍性浸潤など)が検索されている限り、その猫は「HCM表現型」を有するとされる。原因疾患が認められなかった場合、初めてHCMと診断される。³ 本章における猫の心筋疾患は、このACVIM分類体系に基づいて記述する。さらに、読者の理解を容易にするため、また米国心臓協会の提案に従い、⁸ 本章では一次性心筋症を原因不明の心筋症、二次性心筋症を全身性疾患由来または特異的病因因子を有する心筋症として定義する。
In addition to the phenotypical classification, the 2020 ACVIM Consensus Statement proposed a staging system, with the aim to objectively categorize feline patients in the course of their myocardial disease and provide appropriate prognosis and treatment at each stage of illness. This system includes four basic stages (A, B, C, and D) of increasing severity (Table 234.2).
2020年ACVIMコンセンサスステートメントでは、表現型分類に加え、病期分類システムも提唱された。この目的は、猫患者を心筋疾患の進行過程に応じて客観的に分類し、各病期において適切な予後評価および治療を提供することにある。このシステムには、重症度が増加する4段階(A、B、C、D)が含まれる(表234.2)。
TABLE 234.1 Definition, Main Features and Causes of Feline Cardiomyopathy Phenotypes According to the 2020 ACVIM Consensus Statement on Feline Cardiomyopathies³
表234.1 2020年ACVIM猫心筋症コンセンサスステートメントに基づく猫心筋症フェノタイプの定義、主な特徴および原因³
| PHENOTYPE フェノタイプ | MAIN FEATURES 主な特徴 | MAIN CAUSES 主な原因 |
|---|---|---|
| Hypertrophic cardiomyopathy (HCM) phenotype 肥大型心筋症(HCM)フェノタイプ | Diffuse or regional increased LV wall thickness with a nondilated LV chamber, in the absence of congenital or acquired cardiac disease capable of causing the observed magnitude of hypertrophy. Histologic lesions typically include myofiber disarray, intramural arterial arteriosclerosis, and interstitial fibrosis. 観察される程度の肥大を引き起こし得る先天性または後天性心疾患が存在しない状況で、拡張していないLV腔を伴うび漫性または局所性のLV壁厚増加を示す。組織学的病変としては、典型的に心筋線維の錯綜配列、壁内動脈硬化、および間質線維化が含まれる。 |
・HCM ・HCM ・Systemic arterial hypertension ・全身性動脈性高血圧 ・Hyperthyroidism ・甲状腺機能亢進症 ・Reduced preload ・前負荷低下 ・Neoplastic infiltration ・腫瘍性浸潤 ・Transient myocardial thickening ・一過性心筋肥厚 ・Myocarditis ・心筋炎 ・Acromegaly ・先端巨大症 |
| Restrictive cardiomyopathy (RCM) phenotype 拘束型心筋症(RCM)フェノタイプ |
Myocardial form 心筋型 Relatively normal LV dimensions (diameters, wall thicknesses) with LA or biatrial enlargement. LA拡大または両心房拡大を伴い、LV径および壁厚は比較的正常である。 Endomyocardial form 心内膜心筋型 Prominent endocardial scar usually bridging the IVS and LV free wall, potentially causing mid-LV obstruction, and most often associated with LA or biatrial enlargement. More rarely: diffuse endomyocardial scar reducing the LV cavity. 顕著な心内膜瘢痕が通常IVSとLV自由壁を架橋し、中部LV閉塞を引き起こす可能性があり、多くはLA拡大または両心房拡大を伴う。より稀には、び漫性心内膜心筋瘢痕によりLV腔が縮小する。 |
・RCM ・RCM ・Hyperthyroidism ・甲状腺機能亢進症 |
| Dilated cardiomyopathy (DCM) phenotype 拡張型心筋症(DCM)フェノタイプ | LV systolic dysfunction characterized by progressive increase in LV diameter and volume, normal or reduced LV wall thickness, and atrial dilation. LV径および容積の進行性増加、正常または低下したLV壁厚、ならびに心房拡張を特徴とするLV収縮機能障害。 |
・DCM ・DCM ・End-stage HCM ・末期HCM ・Dietary taurine deficiency ・食餌性タウリン欠乏 ・Tachycardia-induced cardiomyopathy ・頻拍誘発性心筋症 ・ARVC with LV involvement ・LV病変を伴うARVC |
| Arrhythmogenic right ventricular cardiomyopathy (ARVC) phenotype 不整脈原性右室心筋症(ARVC)フェノタイプ | Severe RA and RV dilation, often with RV systolic dysfunction and RV wall thinning, as well as arrhythmias and/or right-sided congestive heart failure. 重度のRAおよびRV拡張を示し、しばしばRV収縮機能障害およびRV壁菲薄化を伴い、不整脈および/または右心性うっ血性心不全も伴う。 | ・ARVC ・ARVC |
| Nonspecific phenotype 非特異的フェノタイプ | Phenotype that does not fit well into any of the 4 other phenotypes. In that case, cardiac morphology and function should be described in detail. 他の4つのフェノタイプのいずれにも十分に適合しないフェノタイプ。この場合、心臓の形態および機能を詳細に記載すべきである。 |
ACVIM:米国内科獣医学会(American College of Veterinary Internal Medicine)。IVS:心室中隔。LA:左心房。LV:左心室。RA:右心房。RV:右心室。
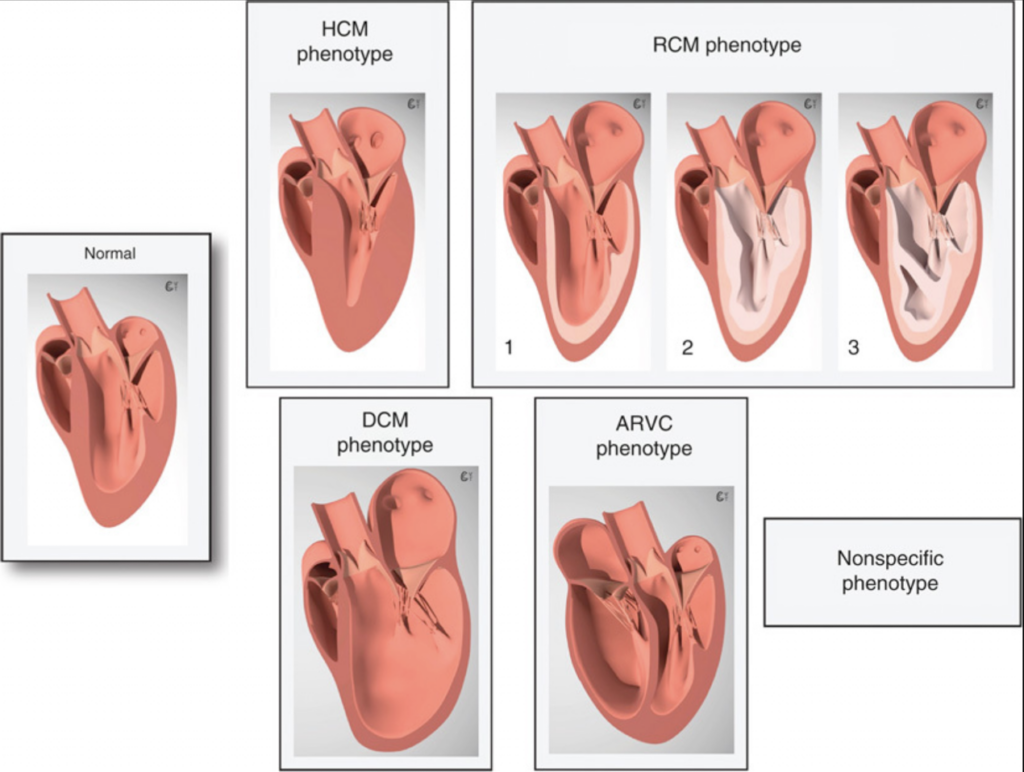
図234.1 猫の心筋症フェノタイプ。³ 猫の心筋症には、既知または未知の原因による5つの異なるフェノタイプが存在し、それらは肥大型心筋症(HCM)フェノタイプ、拘束型心筋症(RCM)フェノタイプ、拡張型心筋症(DCM)フェノタイプ、不整脈原性右室心筋症(ARVC)フェノタイプ、および非特異的フェノタイプである。RCMフェノタイプには、心筋型(1)および心内膜心筋型(2、3)¹⁶が含まれる。後者では、左心室(LV)腔を縮小させるび漫性心内膜心筋瘢痕(2)や、心室中隔とLV自由壁を連結する著明な架橋性瘢痕(3)を認めることがある(表234.1)。Chetboul VおよびTaton C編 Encyclopédie d’imagerie cardiovasculaire ultrasonore du chien et du chat より転載。Issy-les-Moulineaux:772頁。2018年 Elsevier Masson SAS。無断転載禁止。
TABLE 234.2 ACVIM Staging of Feline Cardiomyopathies³
TABLE 234.2 猫の心筋症に対するACVIMステージ分類³
| STAGES ステージ | MAIN FEATURES 主な特徴 | SUBSTAGES サブステージ | ADDITIONAL FEATURES 追加所見 |
|---|---|---|---|
| Stage A ステージA | Cats predisposed to cardiomyopathy 心筋症の素因を有する猫 | ||
| Stage B ステージB | Cats with cardiomyopathy, but without current or previous CHF/ATE Risk for imminent CHF or ATE 心筋症を有するが、現在または過去にCHF/ATEを認めない猫 切迫したCHFまたはATEのリスク | ||
| Low 低い | Stage B1 ステージB1 | Normal atrial size or mild atrial enlargement and no risk factors characterizing stage B2 心房サイズが正常、または軽度心房拡大であり、ステージB2を特徴づけるリスク因子を認めない | |
| Higher 高い | Stage B2 ステージB2 | Moderate or severe atrial enlargement and/or other risk factors (i.e., gallop sound, arrhythmias, decreased LA function, extreme LV hypertrophy, LV systolic dysfunction, spontaneous echo-contrast, thrombus, regional wall motion abnormalities) 中等度または重度の心房拡大、および/またはその他のリスク因子(すなわち、ギャロップ音、不整脈、LA機能低下、極度のLV肥大、LV収縮機能障害、自発性エコーコントラスト、血栓、局所壁運動異常) | |
| Stage C ステージC | Cats with cardiomyopathy and current or previous CHF/ATE 心筋症を有し、現在または過去にCHF/ATEを認める猫 | ||
| Stage D ステージD | Cats with cardiomyopathy and refractory CHF 心筋症を有し、難治性CHFを認める猫 | ||
ACVIM:米国獣医内科学会。ATE:動脈血栓塞栓症。CHF:うっ血性心不全。LA:左心房。LV:左心室。
PREVALENCE:有病率
Primary cardiomyopathies are the most common feline heart diseases, and therefore constitute the central part of this chapter. In a study of 408 cats that underwent a cardiac exam, congenital heart disease was diagnosed in only 12% of the cases; in the remaining 88%, myocardial diseases represented 80% of these, and HCM was by far the most common (68%).²⁰ Similarly, in a report focusing on HCM, RCM and secondary cardiomyopathies, HCM represented 53% of the included cases vs. 15% and 32% for RCM and secondary cardiomyopathies, respectively.²¹ In another study on primary cardiomyopathies,²² HCM was also by far the most common disease (58%), followed by RCM (21%), DCM (10%) and NSCM (10%), with no reported case of ARVC (the rarest feline primary cardiomyopathy). In the latter report, one cat showed echocardiographic changes compatible with so-called moderator band “cardiomyopathy.” Left ventricular (LV) moderator bands, also named false tendons, are cordlike structures of varying length stretching across the LV cavity, attached to the interventricular septum (IVS), LV free wall (LVFW), and/or LV papillary muscles and apex, and composed of varying amounts of Purkinje fibers, collagenous fibers, myocardial and fibrous connective tissue, adipose tissue, and blood vessels covered with endothelium.²³⁻²⁸ As in people,²³⁻²⁵ false tendons are common incidental echocardiographic findings in cats, with no consequence on cardiac morphology and function, except for focal thickening at their myocardial insertion (Figure 234.2, A and B).²⁸⁻³⁰ However, similarly to people,²³ excessive networks of LV moderator bands have been reported in the cat in association with various secondary deleterious effects, such as LV myocardial dysfunction and LV remodeling, arrhythmias, congestive heart failure (CHF), and arterial thromboembolism (ATE), potentially leading to death even in kittens (Figure 234.2, C and D; Videos 234.1 and 234.2).¹˒²⁶˒²⁷ As LV moderator bands are of congenital origin, the term “moderator band cardiomyopathy” commonly used for defining this diseased state, does not strictly fit into the definition of cardiomyopathies.³˒⁸˒¹¹ Nevertheless, the prevalence of false tendons in the left ventricular outflow tract (LVOT) is higher in cats with obstructive hypertrophic cardiomyopathy (OHCM) compared to healthy cats and cats with non-obstructive HCM, which suggests a possible role of false tendons in the pathogenesis of dynamic left ventricular outflow tract obstruction (LVOTO; Figure 234.2, E).²⁹
一次性心筋症は猫における最も一般的な心疾患であり、そのため本章の中心的内容を構成する。心臓検査を受けた408頭の猫を対象とした研究では、先天性心疾患はわずか12%に認められたのみであり、残る88%では心筋疾患がその80%を占め、その中でもHCMが圧倒的に最多(68%)であった。²⁰同様に、HCM、RCM、および二次性心筋症に焦点を当てた報告では、HCMが53%を占め、RCMおよび二次性心筋症はそれぞれ15%、32%であった。²¹別の一次性心筋症に関する研究でも、²² HCMが最も多く(58%)、続いてRCM(21%)、DCM(10%)、NSCM(10%)であり、ARVC(猫において最も稀な一次性心筋症)は報告されなかった。後者の報告では、1頭の猫において、いわゆるモデレーターバンド「心筋症」と一致する心エコー検査所見が認められた。左室モデレーターバンドは偽腱索とも呼ばれ、左室腔を横断する索状構造物であり、心室中隔(IVS)、左室自由壁(LVFW)、および/または左室乳頭筋や心尖部に付着する。これらは長さがさまざまであり、プルキンエ線維、膠原線維、心筋性および線維性結合組織、脂肪組織、内皮で覆われた血管などから構成される。²³⁻²⁸ヒトと同様に、²³⁻²⁵ 偽腱索は猫においても一般的な偶発的心エコー検査所見であり、付着部に局所的肥厚を生じる以外には、心形態や機能に影響を及ぼさない(図234.2 A、B)。²⁸⁻³⁰しかし、ヒトと同様に、²³ 左室モデレーターバンドの過剰なネットワークは、左室心筋機能障害、左室リモデリング、不整脈、うっ血性心不全(CHF)、動脈血栓塞栓症(ATE)など、さまざまな二次的有害影響と関連して猫でも報告されており、子猫においても死亡に至る可能性がある(図234.2 C、D;Videos 234.1および234.2)。¹˒²⁶˒²⁷左室モデレーターバンドは先天性起源であるため、この病態を定義する際によく用いられる「モデレーターバンド心筋症」という用語は、厳密には心筋症の定義には適合しない。³˒⁸˒¹¹それにもかかわらず、左室流出路(LVOT)における偽腱索の有病率は、健常猫や非閉塞性HCM猫と比較して、閉塞性肥大型心筋症(OHCM)猫で高く、偽腱索が動的左室流出路閉塞(LVOTO)の病因形成に関与する可能性が示唆されている(図234.2 E)。²⁹
Lastly, although usually considered an “unclassified cardiomyopathy” in human cardiology, ventricular non-compaction is actually a congenital myocardial disease resulting from an arrest in embryogenesis.⁷˒⁸˒¹¹ It is characterized by prominent myocardial trabeculae and deep inter-trabecular recesses, occurring as an isolated finding or in association with various congenital heart diseases.⁷˒⁸˒¹¹ Biventricular noncompaction has been reported as an extremely rare pathological condition in the cat.³¹˒³²
最後に、ヒト循環器学では通常「未分類心筋症」とみなされているものの、心室非緻密化は実際には胚発生停止に起因する先天性心筋疾患である。⁷˒⁸˒¹¹これは顕著な心筋肉柱および深い肉柱間陥凹を特徴とし、単独所見として、あるいはさまざまな先天性心疾患に伴って認められる。⁷˒⁸˒¹¹両心室性非緻密化は、猫では極めて稀な病的状態として報告されている。³¹˒³²
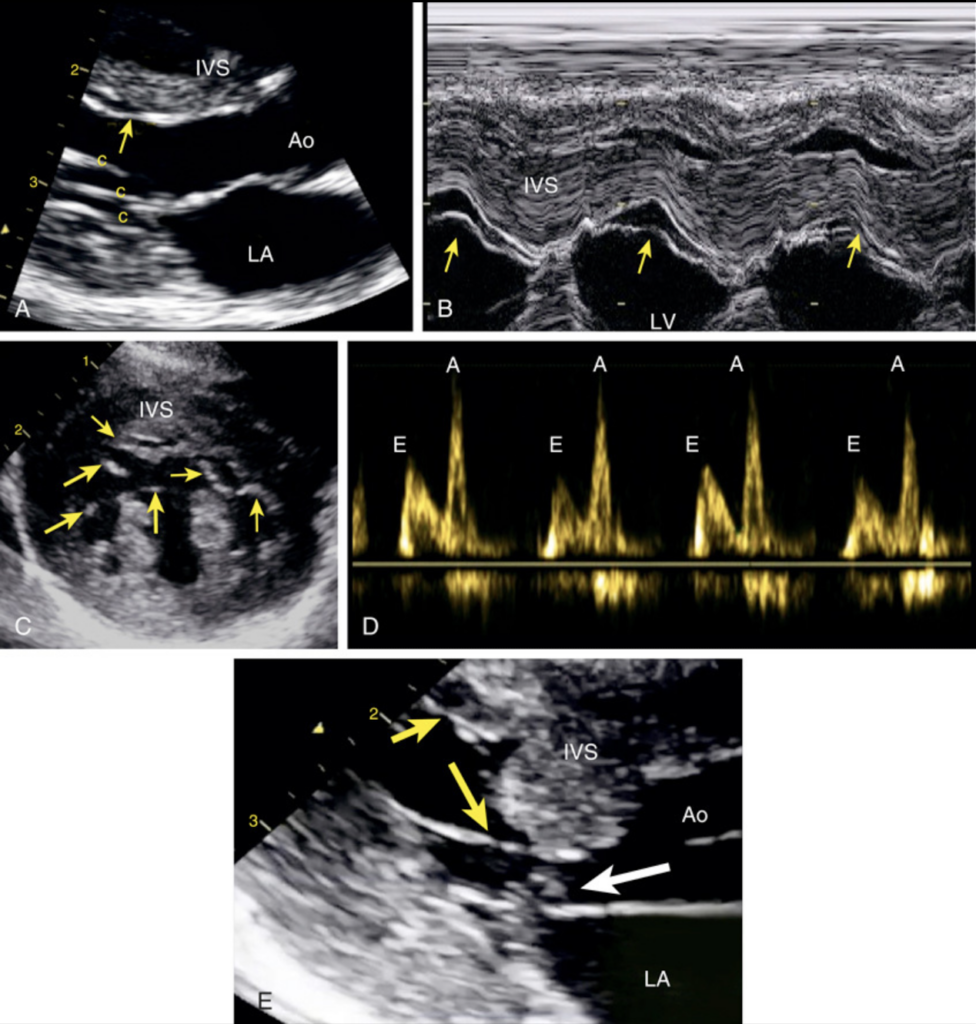
図234.2 左心室仮腱索の心エコー図所見。A-B:仮腱索は通常、細い高エコー性線状構造(矢印)として認められ、拡張期ではより緊張し、収縮期ではより弛緩して見える。本図では、健康な猫における偶発所見として認められている(A:2D法、B:Mモード法)。C-D:左心室(LV)内に過剰な仮腱索ネットワーク(矢印)を示す経心室短軸像。症例は8か月齢のベンガル猫(C)。これは拡張機能異常(D)を伴っており、僧帽弁流入波形における早期流入波(E)/後期流入波(A)比が1未満(E:A = 0.66)であり、さらにE波減速時間が延長(>100 ms、132 ms)していることから、弛緩障害パターンを示している。⁷⁴ E:重度の閉塞性肥大型心筋症を有する本症例では、心室中隔(IVS)が左室流出路(LVOT)内へ突出している。仮腱索(黄色矢印)は大動脈弁下のIVSに付着しており、さらに僧帽弁の収縮期前方運動(白矢印)が認められ、これらの両者がLVOT閉塞を悪化させている。Ao:大動脈。c:腱索。LA:左心房。
CLINICAL AND MORPHOLOGIC CHARACTERISTICS:臨床的および形態学的特徴
HYPERTROPHIC CARDIOMYOPATHY:肥大型心筋症
HCM is characterized phenotypically by increased cardiac mass due to a hypertrophied non-dilated LV in the absence of an obvious cause of left ventricular hypertrophy (LVH), the most common of which are systemic arterial hypertension and hyperthyroidism (Table 234.1).¹˒³˒³³
HCMは、左室肥大(LVH)の明らかな原因が存在しない状況下において、肥厚し非拡張性となった左心室(LV)により心筋量が増加することを特徴とする表現型である。LVHの最も一般的な原因としては、全身性動脈性高血圧および甲状腺機能亢進症が挙げられる(表234.1)。¹˒³˒³³
Left Ventricular Hypertrophic Patterns, Macroscopic/Microscopic Features:左室肥大パターン、肉眼的/顕微鏡的特徴
As in people, feline HCM is characterized by marked phenotypic variability, including mild to severe, diffuse or segmental, concentric LVH (Figures 234.3 and 234.4).³³⁻³⁶ In up to two-thirds of cats with HCM, LVH is diffuse, involving portions or all of both the IVS and the LVFW, with hypertrophy of the left papillary muscles and a consequently reduced LV cavity (Video 234.3).³³˒³⁶ Diffuse LVH can be symmetric or asymmetric with predominant thickening of the IVS or LVFW. In about one-third of cases, LVH is confined to only one segment, e.g., usually the basal IVS and less commonly the apex.³³˒³⁶ In some cases, the thickened basal IVS protrudes into the LVOT, resulting in mild to severe LVOTO, thus defining OHCM forms (Video 234.4). Marked combined LVH and papillary muscle hypertrophy can result in systolic mid-ventricular cavity obstruction, associated with the presence of endocardial contact plaques.²˒³⁷ Although rare, myocardial infarction of the LVFW may also occur (Video 234.5).³³ Such varied geometric patterns are also revealed by two-dimensional (2D) and M-mode echocardiography, with breed variations.³⁸˒³⁹ In one study of cats with HCM, Persian and Chartreux cats showed significantly more OHCM (44%) than did cats of other breeds (18%), whereas almost half of Maine Coon cats had diffuse symmetric LVH.³⁹
ヒトと同様に、猫のHCMは顕著な表現型の多様性を特徴とし、軽度から重度まで、び漫性あるいは区域性、求心性LVHを示す(図234.3および234.4)。³³⁻³⁶ HCM猫の最大3分の2では、LVHはび漫性であり、心室中隔(IVS)および左室自由壁(LVFW)の一部または全体に及び、さらに左乳頭筋肥大を伴い、その結果左室腔は縮小する(Video 234.3)。³³˒³⁶び漫性LVHは対称性または非対称性を示し、IVSまたはLVFWの優位な肥厚を伴う。約3分の1の症例では、LVHは単一区域のみに限局し、通常は基部IVSに認められ、まれに心尖部に認められる。³³˒³⁶ 一部の症例では、肥厚した基部IVSが左室流出路(LVOT)内へ突出し、軽度から重度の左室流出路閉塞(LVOTO)を生じることで、閉塞性肥大型心筋症(OHCM)型を形成する(Video 234.4)。著明なLVHと乳頭筋肥大の併発により、収縮期中部左室腔閉塞を生じることがあり、これは心内膜接触プラークの存在を伴う。²˒³⁷ まれではあるが、LVFWの心筋梗塞も発生しうる(Video 234.5)。³³このような多様な幾何学的パターンは、二次元(2D)およびMモード心エコー検査によっても明らかとなり、品種差が存在する。³⁸˒³⁹ HCM猫を対象としたある研究では、ペルシャおよびシャルトリューでは、他品種(18%)と比較してOHCMが有意に多く(44%)、一方メインクーンの約半数ではび漫性対称性LVHが認められた。³⁹
In cases of mild to moderate LVH, the left atrium (LA) is usually normal.² Severe LVH is often associated with mild to severe left atrial enlargement (LAE; Figure 234.3).³³ Right ventricular (RV) hypertrophy and dysfunction occur in some cats with HCM (with or without right atrial [RA] enlargement) and seem to be associated with clinical severity.⁴⁰
軽度から中等度のLVH症例では、左心房(LA)は通常正常である。² 重度LVHでは、軽度から重度の左心房拡大(LAE)を伴うことが多い(図234.3)。³³ また、一部のHCM猫では右室(RV)肥大および右室機能障害が認められ(右心房[RA]拡大の有無を問わない)、これは臨床的重症度と関連していると考えられている。⁴⁰
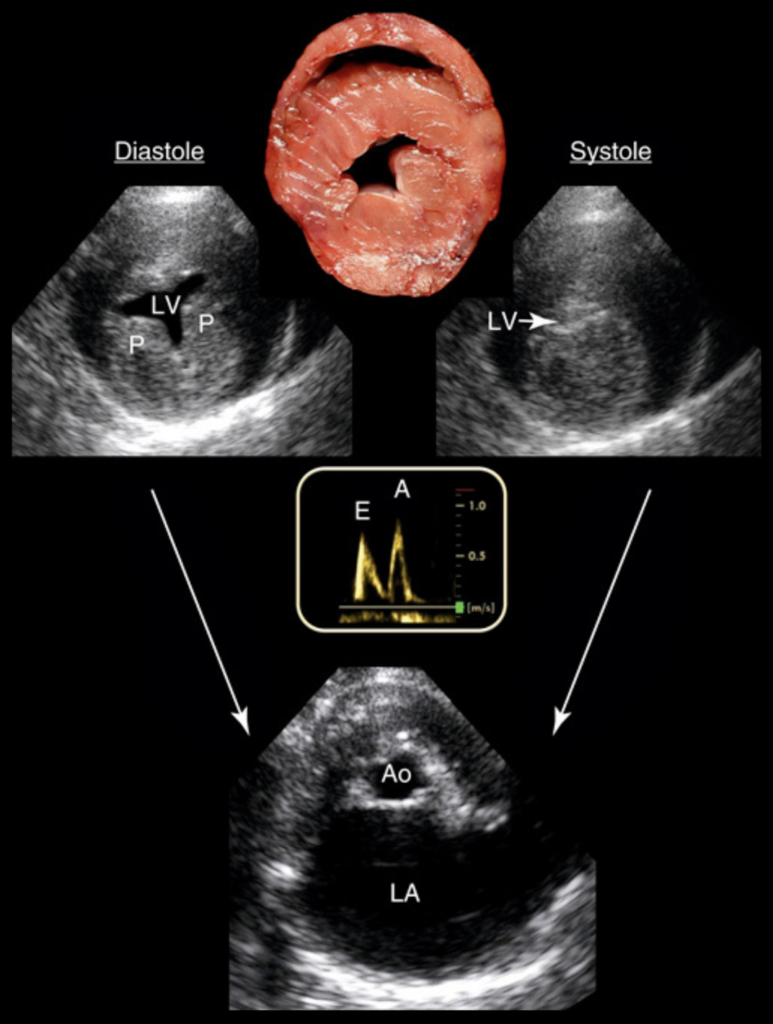
図234.3 肥大型心筋症:びまん性かつ対称性の左心室(LV)肥大を有する猫における肉眼像、心エコー像、およびドプラ所見。横断切片の肉眼標本および右傍胸骨短軸像(上段図)はいずれも重度のLV肥大を示しており、その結果としてLV内腔は著しく縮小している。収縮終期にはLV腔は認められない。二次的に著明な左心房(LA)拡大も認められる(下段;拡張終期LA:Ao = 3.7、基準範囲0.5–1.2)。⁸⁸ 僧帽弁通過血流のパルスドプラ検査(中央図)では、LV弛緩障害パターンが認められる。逆転した(<1)E:A比は、弛緩障害による早期LV流入低下と、LA収縮によるLV充満へのLA寄与増加の両方を示している。⁷⁴ Ao:大動脈。LV:左心室。P:左室乳頭筋。肉眼病理画像提供:Prof. Jean-Jacques Fontaine(フランス・アルフォール国立獣医学校病理学部門)。
図234.4 猫肥大型心筋症における表現型の多様性。猫の肥大型心筋症は、びまん性対称性左心室肥大および非対称性左心室肥大(LVH)を含む、さまざまな左心室(LV)幾何学的パターンを特徴とする。大動脈弁下心室中隔(IVS)肥大は、単独で認められる場合もあれば、びまん性LVHパターンに関連して認められる場合もある。LV乳頭筋肥大もしばしば存在する。これらすべての形態は、ここに示されるように左心房拡大および肺静脈うっ血を引き起こし得る。左下:比較のため正常例を示す。LVFW:左心室自由壁。Chetboul VおよびTaton C編『Encyclopédie d’imagerie cardiovasculaire ultrasonore du chien et du chat』より転載。Issy-les-Moulineaux、772頁、2018年、Elsevier Masson SAS。All rights reserved.
Histopathology:組織病理学
As in people,³⁵ histological features of feline HCM include various degrees of myocardial fiber disarray within the LV myocardium (less commonly the RV myocardium), associated with mild to severe arteriosclerosis of intramural coronary arteries, interstitial myocardial fibrosis, and replacement fibrosis (Figure 234.5).²˒³³˒³⁴˒³⁶ In one report, disorganized cardiac muscle cells were identified in the IVS of 30% of HCM cats. Disorganized architecture of the LVFW was less common (14%) and consistently associated with IVS disorganization.³⁴ Such histological differences impact regional diastolic myocardial function, as observed using tissue Doppler imaging (TDI).⁴¹˒⁴² In both people and cats, myocardial fiber disorganization can also be observed in non-severely thickened, even in non-hypertrophied, LV myocardial segments,² which from a practical point of view, explains why TDI can detect regional myocardial dysfunction in apparently normal myocardial segments of HCM cats (Figure 234.6).⁴¹ In OHCM, an LVOT fibrous contact plaque can be observed on the IVS surface due to systolic apposition of the mitral valve (MV) leaflets to the IVS. Increased myocardial collagen deposition, associated with neutrophilic and lymphocytic infiltrates, has also been found in the myocardium of cats with pre-clinical HCM. This suggests the possible contribution of an early inflammatory process to myocardial fibrosis (e.g., involving inflammatory cytokines).⁴³
ヒトと同様に、³⁵ 猫HCMの組織学的特徴には、LV心筋(よりまれにRV心筋)内におけるさまざまな程度の心筋線維錯綜配列が含まれ、さらに壁内冠動脈の軽度から重度の動脈硬化、間質性心筋線維化、および置換性線維化を伴う(図234.5)。²˒³³˒³⁴˒³⁶ある報告では、HCM猫の30%においてIVS内に配列異常を示す心筋細胞が確認された。LVFWにおける構築異常はより少なく(14%)、常にIVSの構築異常と関連していた。³⁴このような組織学的差異は、組織ドプラ法(TDI)で観察されるように、局所的拡張機能へ影響を及ぼす。⁴¹˒⁴² ヒトおよび猫の双方において、心筋線維配列異常は、重度に肥厚していない、さらには肥大していないLV心筋区域でも認められることがあり、² 実際的観点からは、これによりTDIが、一見正常に見えるHCM猫の心筋区域において局所的心筋機能障害を検出できる理由が説明される(図234.6)。⁴¹OHCMでは、僧帽弁(MV)弁尖が収縮期にIVSへ接触することにより、IVS表面にLVOT線維性接触プラークが認められる場合がある。さらに、好中球およびリンパ球浸潤を伴う心筋コラーゲン沈着増加が、前臨床期HCM猫の心筋でも確認されている。これは、炎症性サイトカインを含む初期炎症過程が心筋線維化へ寄与する可能性を示唆している。⁴³
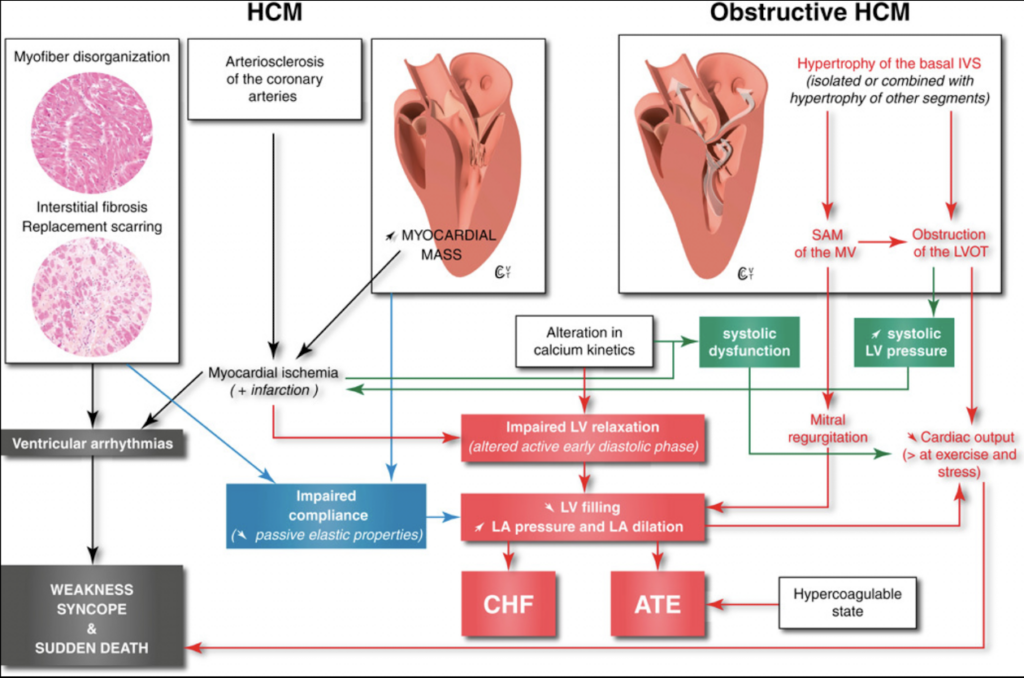
図234.5 猫肥大型心筋症の主要な病態生理学的帰結。(1) 拡張機能障害。能動的心筋弛緩および受動的コンプライアンスの異常は、左心室(LV)充満異常を引き起こす:拡張終期容量(EDV)の低下、あるいはEDVは保たれていても充満圧は上昇する。⁷⁴ 肥大型心筋症(HCM)では、弛緩能およびコンプライアンスの両方が障害されるが、弛緩異常が優位であり早期から出現し、初期急速LV充満に影響を与える。初期LV充満速度および容量の低下は、代償的に左心房(LA)収縮によるLV充満寄与の増加を引き起こす。これは初期には拡張終期LA圧上昇を伴う。⁷⁴ LVコンプライアンス低下は、LV肥大自体、間質性線維化、置換性瘢痕形成、および心筋細胞配列異常など複数の因子によって生じ、LV拡張期圧および続発するLA圧上昇にも寄与する。後者は病勢進行とともに悪化し、その結果LA拡張を引き起こし、最終的には肺血管系へ逆伝播して静脈うっ血およびうっ血性心不全(CHF)へ至る。LA拡張はまた血流停滞および動脈血栓塞栓症(ATE)の素因ともなり、特にHCM猫ではCHFやATEが存在しなくても全身性過凝固状態が確認されている。⁷⁸˒⁷⁹
(2) 主体的ではないものの、心筋虚血、Ca²⁺動態異常、間質結合組織増加、および局所的心筋不同期に起因する収縮機能障害は、特に終末期疾患あるいは閉塞性HCMにおいて、心拍出量低下に寄与し得る。⁴¹˒⁴²˒⁸⁰
(3) HCMの組織病理学的病変は、リエントリー性心室頻拍性不整脈の電気的不安定基盤となり、虚脱、失神、および突然死の原因となる。
(4) 閉塞性HCMでは、動的左室流出路(LVOT)閉塞により高い収縮期心室内圧較差(100 mmHg超となることもある)が生じ、心拍出量低下やLV肥大・虚血悪化(心筋壁応力および酸素需要増加による)など、複数の有害作用を引き起こす。大動脈弁下閉塞は、肥厚した基部心室中隔(IVS)のLVOT内突出と、僧帽弁(MV)の収縮期前方運動(SAM)の両者により生じ、異常な収縮中〜後期のMV-IVS接触(図234.8)を特徴とする。ヒト閉塞性HCMでは、僧帽弁-IVS接触時間が長いほどLVOT閉塞重症度は高い。³⁵˒⁸¹ SAMの存在はまたMV弁尖接合不全を引き起こし、後外側方向へ向かうMV逆流を生じ、それがLA圧上昇へ寄与する可能性がある。³⁵˒⁸¹ 図版作成および構想:Dr. Charlotte Taton、Prof. Valérie Chetboul。組織病理画像提供:Prof. Jean-Jacques Fontaine(フランス・アルフォール国立獣医学校病理学部門)。
HCM:肥大型心筋症
Obstructive HCM:閉塞性肥大型心筋症
Myofiber disorganization:心筋線維配列異常
Arteriosclerosis of the coronary arteries:冠動脈の動脈硬化
Interstitial fibrosis:間質性線維化
Replacement scarring:置換性瘢痕形成
↑ MYOCARDIAL MASS:心筋重量増加
Hypertrophy of the basal IVS (isolated or combined with hypertrophy of other segments):基部心室中隔(IVS)の肥大(単独または他部位肥大を伴う)
SAM of the MV:僧帽弁(MV)の収縮期前方運動(SAM)
Obstruction of the LVOT:左室流出路(LVOT)閉塞
Myocardial ischemia (+ infarction):心筋虚血(+梗塞)
Alteration in calcium kinetics:カルシウム動態異常
systolic dysfunction:収縮機能障害
↑ systolic LV pressure:左室収縮期圧上昇
Ventricular arrhythmias:心室性不整脈
Impaired LV relaxation (altered active early diastolic phase):左室弛緩障害(能動的早期拡張期相の異常)
Mitral regurgitation:僧帽弁逆流
Impaired compliance (↘ passive elastic properties):コンプライアンス低下(受動的弾性特性低下)
↘ LV filling ↑ LA pressure and LA dilation:左室充満低下、左心房(LA)圧上昇および左心房拡大
↘ Cardiac output (> at exercise and stress):心拍出量低下(運動時およびストレス時でより顕著)
CHF:うっ血性心不全
ATE:動脈血栓塞栓症
Hypercoagulable state:過凝固状態
WEAKNESS SYNCOPE & SUDDEN DEATH:虚脱、失神、および突然死
Epidemiology:疫学
In large HCM populations, males are overrepresented (70-79%), with a predominance of Domestic Shorthaired cats (DSH, 65-70%), followed by Domestic Longhaired cats (DLH, 9-22%) and Persians (3-12%).³⁹˒⁴⁴˒⁴⁵ Other commonly reported breeds vary according to studies (British Shorthair, Chartreux, Himalayan, Maine Coon, Sphynx, Ragdoll).³⁹˒⁴⁴⁻⁴⁶ Despite sparse published information, Bengal cats appear to be overrepresented as well. Burmese, Siamese, Oriental Shorthairs and Abyssinians are less commonly affected.¹˒³⁹˒⁴⁴˒⁴⁵ Most cats with HCM are middle-aged at diagnosis (median age: 5-7 years), but with wide age ranges ([0.5-19], [0.2-18.3], and [0.2-16.7] years in 3 reports involving 731 cats with HCM)³⁹˒⁴⁴˒⁴⁵ and breed representation. In one report, Maine Coon and Sphynx cats were younger at diagnosis than other cats (Figure 234.7, A).³⁹ In another, Ragdoll cats were younger (2.5 [0.5-4.5] years) than others (5.0 [0.2-16.7] years).⁴⁵ Interestingly, HCM has been shown to be common in apparently healthy cats, with an estimated global prevalence of 15%; this increases significantly with age, i.e., 4.3% (6-12 months), 9.9% (1-3 years old), 18.6% (3-9 years old), and 29.4% (≥9 years old).⁴⁷
大規模HCM集団では、雄が過剰代表されており(70〜79%)、ドメスティック・ショートヘアー(DSH、65〜70%)が最多であり、続いてドメスティック・ロングヘアー(DLH、9〜22%)、ペルシャ(3〜12%)が多い。³⁹˒⁴⁴˒⁴⁵その他よく報告される品種は研究によって異なり、ブリティッシュショートヘアー、シャルトリュー、ヒマラヤン、メインクーン、スフィンクス、ラグドールなどが含まれる。³⁹˒⁴⁴⁻⁴⁶公表情報は限られているものの、ベンガルも過剰代表されているようである。一方、バーミーズ、シャム、オリエンタルショートヘアー、アビシニアンでは罹患頻度は低い。¹˒³⁹˒⁴⁴˒⁴⁵HCM猫の多くは診断時に中年齢(中央値5〜7歳)であるが、年齢範囲は広く、HCM猫731頭を含む3報告では、それぞれ0.5〜19歳、0.2〜18.3歳、0.2〜16.7歳であった。³⁹˒⁴⁴˒⁴⁵ また、年齢分布には品種差も存在する。ある報告では、メインクーンおよびスフィンクスは他品種より若齢で診断されていた(図234.7 A)。³⁹ 別の報告では、ラグドールは他品種(5.0[0.2〜16.7]歳)より若齢(2.5[0.5〜4.5]歳)であった。⁴⁵興味深いことに、HCMは一見健康な猫にも一般的に認められ、推定全体有病率は15%である。この有病率は加齢とともに著明に増加し、6〜12か月齢で4.3%、1〜3歳で9.9%、3〜9歳で18.6%、9歳以上で29.4%である。⁴⁷
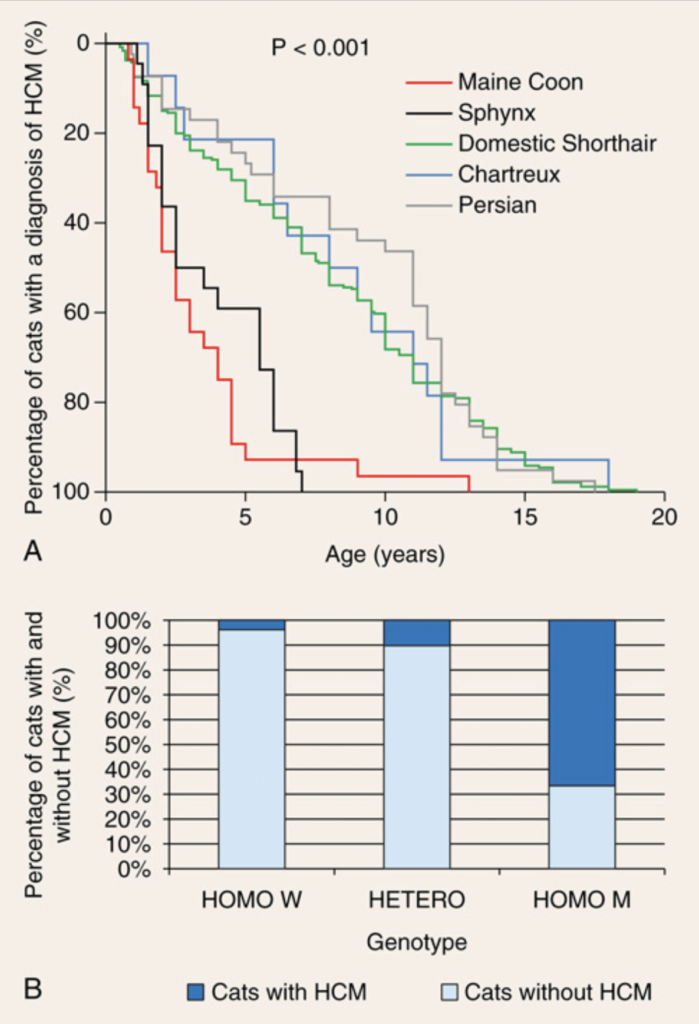
Feline hypertrophic cardiomyopathy: breed specificities.
猫肥大型心筋症:品種特異性。
A, Age at the time of diagnosis in 344 cats with hypertrophic cardiomyopathy (HCM) (239 Domestic Shorthairs, 41 Persians, 22 Sphynx, 28 Maine Coons, and 14 Chartreux).³⁹
A、肥大型心筋症(HCM)と診断された344頭の猫(ドメスティックショートヘア239頭、ペルシャ41頭、スフィンクス22頭、メインクーン28頭、シャルトリュー14頭)における診断時年齢。³⁹
B, Distribution of 96 Maine Coon cats according to genotype (Homo W, Hetero, Homo M) and phenotype (presence or absence of HCM).⁴²
B、遺伝子型(Homo W、Hetero、Homo M)および表現型(HCMの有無)に基づく96頭のメインクーン猫の分布。⁴²
HOMO W group: homozygous wild-type cats, i.e., without the MyBPC3-A31P mutation.
HOMO W群:MyBPC3-A31P変異を有さないホモ接合野生型猫。
HETERO and HOMO M groups, respectively: heterozygous and homozygous mutated cats for the MyBPC3-A31P mutation.
HETERO群およびHOMO M群は、それぞれMyBPC3-A31P変異のヘテロ接合変異猫およびホモ接合変異猫である。
Genetic Basis—Relationship Between Genotype and Phenotype:遺伝的基盤―遺伝子型と表現型の関係
Human HCM:ヒトHCM
Human HCM is a familial disease in at least 50-60% of cases, with autosomal dominant inheritance most commonly identified.⁴⁸˒⁴⁹ HCM was the first human heart disease for which a molecular genetic cause was demonstrated, with the responsible gene (MYH7, coding for the beta-myosin heavy chain protein) having been identified in 1990.⁵⁰ At the time of this writing, more than 1500 mutations associated with HCM have been identified, with most implicated genes encoding for sarcomere proteins.⁴⁸˒⁴⁹
ヒトHCMは少なくとも50〜60%の症例で家族性疾患であり、最も一般的な遺伝形式は常染色体優性遺伝である。⁴⁸˒⁴⁹HCMは、分子遺伝学的原因が解明された最初のヒト心疾患であり、その原因遺伝子(βミオシン重鎖蛋白をコードするMYH7)が1990年に同定された。⁵⁰本稿執筆時点で、HCMに関連する1500を超える変異が同定されており、その多くはサルコメア蛋白をコードする遺伝子である。⁴⁸˒⁴⁹
Maine Coon Breed:メインクーン種
A mutation in the cardiac sarcomeric myosin binding protein C gene (MyBPC3) that causes inherited HCM, with autosomal dominant inheritance, was similarly identified in the Maine Coon breed in 2005.⁵¹ It was the first report to demonstrate a spontaneous mutation causing HCM in a non-human species.⁵¹ The MyBPC3 gene was shown to be mutated in exon 3, with a single base pair change (guanine to cytosine) causing an alteration of the protein structure, owing to the replacement of one conservative amino acid (i.e., alanine, in the 31st codon) by proline.⁵¹ In a study of 3310 cats of 17 different breeds from Asia, Europe, Australia, and North America, involving 3238 Maine Coon cats, the latter accounted for 100% of all 1089 cats positive for the MyBPC3-A31P mutation.⁵² Similarly, a European report involving 3757 cats of 17 different breeds, including 2744 Maine Coons, identified the mutation only in Maine Coon cats and one British Longhair.⁵³ Thus the MyBPC3-A31P substitution mutation appears to be specific to the Maine Coon breed, although potential marginal events may occur.⁵²˒⁵³ In the late 2000s, the prevalence of the mutation in this breed was high, ranging from 31% (Asia, North America) to 42% (Europe) and 46% (Australia), with a marked predominance (up to 92%) of the heterozygous status, the current prevalence being unknown.⁵²˒⁵³ The prevalence of HCM is strongly dependent on genetic status (Figure 234.7, B).⁵³˒⁵⁴ The MyBPC3-A31P mutation is associated with an increased risk of HCM (relative risk [RR] = 9.9) and the risk is much higher (RR = 35.5) for cats that are homozygous for the mutation. Incomplete penetrance has been documented in middle-aged cats that are heterozygous for the mutation.⁵³˒⁵⁴ In one study, >80% of heterozygous cats remained healthy at least until 4 years of age.⁴² Conversely, some homozygous wild-type Maine Coon cats may develop HCM, indicating involvement of other causes or mutations.⁴²˒⁵⁴˒⁵⁵ This was recently confirmed by the identification of a novel mutation in the TNNT2 gene (encoding for the cardiac-specific sarcomeric protein cardiac troponin-T) associated with HCM in a Maine Coon cat.⁵⁶
2005年、メインクーンにおいても、常染色体優性遺伝形式を示す遺伝性HCMの原因として、心筋サルコメア・ミオシン結合蛋白C遺伝子(MyBPC3)の変異が同定された。⁵¹ これは、ヒト以外の種において自然発生変異がHCMを引き起こすことを示した最初の報告であった。⁵¹MyBPC3遺伝子ではエクソン3に変異が存在し、1塩基対置換(グアニン→シトシン)により蛋白構造変化が生じ、31番コドンの保存的アミノ酸であるアラニンがプロリンへ置換されることが示された。⁵¹アジア、ヨーロッパ、オーストラリア、北米の17品種3310頭(うち3238頭がメインクーン)を対象とした研究では、MyBPC3-A31P変異陽性1089頭の100%がメインクーンであった。⁵²同様に、17品種3757頭(うち2744頭がメインクーン)を対象とした欧州報告では、この変異はメインクーンおよび1頭のブリティッシュロングヘアーでのみ認められた。⁵³したがって、MyBPC3-A31P置換変異は主としてメインクーン特異的変異と考えられるが、境界的例外の可能性は存在する。⁵²˒⁵³2000年代後半には、この変異の保有率は高く、アジア・北米で31%、ヨーロッパで42%、オーストラリアで46%であり、その大多数(最大92%)はヘテロ接合体であった。現在の有病率は不明である。⁵²˒⁵³HCM有病率は遺伝学的状態に強く依存する(図234.7 B)。⁵³˒⁵⁴ MyBPC3-A31P変異はHCMリスク増加(相対危険度[RR]=9.9)と関連し、ホモ接合体ではそのリスクはさらに高い(RR=35.5)。また、ヘテロ接合体中年齢猫においては不完全浸透が報告されている。⁵³˒⁵⁴ ある研究では、ヘテロ接合体猫の80%以上が少なくとも4歳までは健康を維持していた。⁴²一方で、野生型ホモ接合体メインクーンでもHCMを発症する場合があり、他の原因または変異の関与が示唆される。⁴²˒⁵⁴˒⁵⁵これは最近、HCMを有するメインクーンで、心筋特異的サルコメア蛋白である心筋トロポニンTをコードするTNNT2遺伝子の新規変異が同定されたことで裏付けられた。⁵⁶
Other Feline Breeds:その他の猫品種
A second substitution mutation in MyBPC3 has been identified in association with HCM in the Ragdoll breed.⁵⁷ This MyBPC3 R820W mutation is also characterized by a single base pair change (cytosine to thymine in codon 820), with secondary change of one amino acid (arginine to tryptophan).⁵⁷ In a survey of 236 Ragdoll cats, the prevalence of the mutation was 34%, with 85% of these being heterozygous.⁵⁸ Familial forms of HCM have also been reported or suggested in several other breeds, including British Shorthairs,⁴⁶ Sphynx,⁵⁹˒⁶⁰ Norwegian Forest cats,⁶¹ Bengals, and non-pedigree cats.⁶²˒⁶³ An autosomal dominant inheritance pattern with incomplete penetrance has been shown in the Sphynx breed,⁶⁰ and more recently a novel mutation in exon 12 of the ALMS1 gene has been identified in Sphynx with HCM, with a penetrance of 77%.⁶⁴ The Alström syndrome protein 1 (ALMS1) gene encodes for a protein involved in the regulation of cell cycle proliferation in perinatal cardiomyocytes.⁶⁴ The ALMS1 mutation was found in most but not all affected Sphynx cats (87%), suggesting the presence of at least one other HCM-associated mutation in this specific feline breed.⁶⁴ Lastly, a variant in MYH7 has been reported in a DSH cat, but was not found in a population of 103 cats (DSH, DLH, and various pure breeds) with HCM.⁶⁵˒⁶⁶
MyBPC3における第2の置換変異が、ラグドールにおけるHCMと関連して同定されている。⁵⁷ このMyBPC3 R820W変異も、1塩基対置換(820番コドンにおけるシトシン→チミン)を特徴とし、その結果アミノ酸置換(アルギニン→トリプトファン)が生じる。⁵⁷236頭のラグドールを対象とした調査では、この変異の保有率は34%であり、その85%はヘテロ接合体であった。⁵⁸家族性HCMは、ブリティッシュショートヘアー、⁴⁶ スフィンクス、⁵⁹˒⁶⁰ ノルウェージャンフォレストキャット、⁶¹ ベンガル、および雑種猫でも報告または示唆されている。⁶²˒⁶³スフィンクスでは、不完全浸透を伴う常染色体優性遺伝形式が示されており、⁶⁰ さらに最近、HCMスフィンクスにおいてALMS1遺伝子エクソン12の新規変異が同定され、その浸透率は77%であった。⁶⁴Alström syndrome protein 1(ALMS1)遺伝子は、周産期心筋細胞における細胞周期増殖調節に関与する蛋白をコードする。⁶⁴ALMS1変異は多くの罹患スフィンクス(87%)で認められたが、すべてではなく、この品種には少なくとももう1つ別のHCM関連変異が存在することが示唆されている。⁶⁴最後に、MYH7変異がDSH猫で報告されているが、HCMを有する103頭(DSH、DLHおよび各種純血種)の集団では確認されなかった。⁶⁵˒⁶⁶
Pathophysiological Consequences (see detailed explanations in Figure 234.5):病態生理学的結果(詳細は図234.5参照)
Ventricular arrhythmias, myocardial dysfunction and dynamic LVOTO are the main pathophysiological consequences of HCM. Diastolic dysfunction, which is considered the major mechanism explaining the development of CHF, occurs early in the course of HCM; this has been confirmed by TDI, even before detectable chamber remodeling (Figure 234.6).⁴¹˒⁴²˒⁶⁷⁻⁷⁴ It results in progressively increased LA pressure with secondary LAE, and CHF (pulmonary edema). Because visceral pleural veins drain into the LA in cats, increases in LA pressure also can lead to pleural effusion due to a decrease in visceral pleural venous drainage.⁷⁵ As confirmed by decreased blood velocities in the LA appendage,⁷⁶ blood stasis is another common complication of LAE, predisposing to thrombus formation and ATE (Videos 234.6 to 234.9) (ch. 238).⁷⁷⁻⁷⁹ Regional and more rarely global systolic dysfunction may also be present (Figure 234.6).⁴¹˒⁴²˒⁸⁰ Lastly, an abnormal motion of the MV (systolic anterior motion, SAM; Figures 234.5 and 234.8) can contribute to both LVOTO with decreased cardiac output and MV regurgitation (Videos 234.10, 234.11). It is frequently reported in cats with HCM (29-67%).²⁹˒³⁶˒⁴⁴˒⁴⁵˒⁶⁸˒⁸¹ The length of the anterior MV leaflet and prevalence of false tendons in the LVOT are higher in cats with OHCM than in cats with non-obstructive HCM forms (41% vs. 22%), suggesting a possible role of these abnormalities in LVOTO (Figure 234.2).²⁹
心室性不整脈、心筋機能障害、および動的LVOTOが、HCMの主要な病態生理学的結果である。CHF発症の主たる機序と考えられている拡張機能障害は、HCM経過の早期から出現し、これはTDIにより、検出可能な心腔リモデリング以前の段階でも確認されている(図234.6)。⁴¹˒⁴²˒⁶⁷⁻⁷⁴その結果、LA圧は徐々に上昇し、二次的LAEおよびCHF(肺水腫)を生じる。猫では臓側胸膜静脈がLAへ流入するため、LA圧上昇は臓側胸膜静脈ドレナージ低下を介して胸水貯留も引き起こしうる。⁷⁵LA耳介内血流速度低下で確認されるように、⁷⁶ 血液うっ滞もLAEの一般的合併症であり、血栓形成およびATEの素因となる(Videos 234.6〜234.9)(第238章)。⁷⁷⁻⁷⁹局所的、まれには全体的な収縮機能障害も存在しうる(図234.6)。⁴¹˒⁴²˒⁸⁰最後に、MVの異常運動(収縮期前方運動[SAM];図234.5および234.8)は、心拍出量低下を伴うLVOTOおよびMV逆流の双方に寄与する可能性がある(Videos 234.10、234.11)。SAMはHCM猫で高頻度に報告されており(29〜67%)、²⁹˒³⁶˒⁴⁴˒⁴⁵˒⁶⁸˒⁸¹ 前尖MV弁尖長およびLVOT内偽腱索の頻度は、非閉塞性HCMよりOHCMで高率である(41%対22%)。このことは、これら異常構造がLVOTO病態形成に関与する可能性を示唆している(図234.2)。²⁹
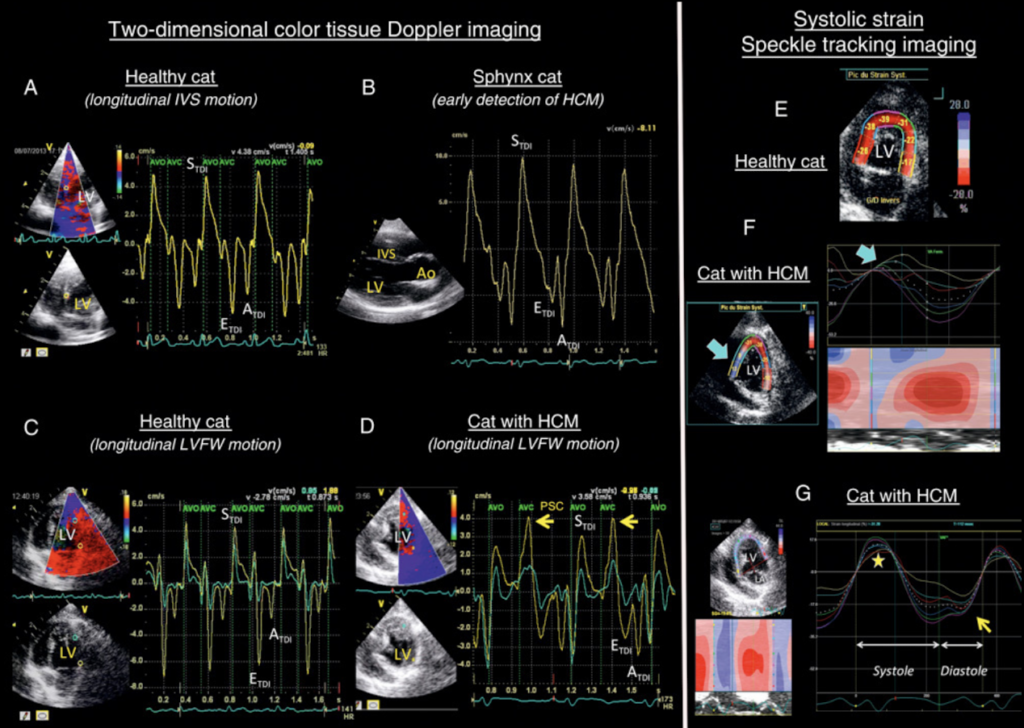
Myocardial dysfunction associated with feline hypertrophic cardiomyopathy: tissue Doppler and speckle tracking imaging.
猫肥大型心筋症に関連する心筋機能障害:組織ドプラ法およびスペックルトラッキングイメージング。
Longitudinal myocardial velocity profiles of the interventricular septum (IVS) (A, B) and the left ventricular free wall (LVFW) (C, D), obtained from left apical long-axis views.
左心尖部長軸像から得られた、心室中隔(IVS)(A, B)および左室自由壁(LVFW)(C, D)の縦方向心筋速度プロファイル。
S_TDI, E_TDI, and A_TDI are peak myocardial velocities recorded during systole, early diastole, and late diastole, respectively.
S_TDI、E_TDI、およびA_TDIは、それぞれ収縮期、拡張早期、および拡張後期に記録された心筋最大速度である。
A-B, Compared to the equivalent in a healthy cat (A), the velocity profile recorded at the IVS base in the Sphynx cat (B) shows a typical diastolic alteration: an inverted E_TDI:A_TDI (E_TDI:A_TDI <1) despite the absence of myocardial hypertrophy on two-dimensional and M-mode echocardiography.
A-B、健常猫(A)と比較して、スフィンクス猫(B)のIVS基部で記録された速度プロファイルでは、典型的な拡張機能異常が認められる。すなわち、二次元およびMモード心エコー検査で心筋肥大を認めないにもかかわらず、逆転したE_TDI:A_TDI(E_TDI:A_TDI <1)がみられる。
Six months later, this cat developed moderate subaortic interventricular septum hypertrophy (IVSH), followed by diffuse asymmetric obstructive hypertrophic cardiomyopathy (HCM).
6か月後、この猫は中等度の大動脈弁下心室中隔肥大(IVSH)を呈し、その後、びまん性非対称性閉塞性肥大型心筋症(HCM)へ進行した。
C-D, Compared to the equivalent in a healthy cat (C), longitudinal velocity profiles recorded at the base (yellow) and apex (green) of the LVFW in a cat with HCM (D) show distinct signs of regional diastolic dysfunction: an inverted E_TDI:A_TDI at the base and post-systolic contraction (PSC) waves (yellow arrows) after S_TDI waves and after aortic valve closure (AVC).
C-D、健常猫(C)と比較して、HCM猫(D)のLVFW基部(黄色)および心尖部(緑色)で記録された縦方向速度プロファイルでは、局所的拡張機能障害を示す明瞭な所見が認められる。すなわち、基部における逆転したE_TDI:A_TDIおよび、S_TDI波後かつ大動脈弁閉鎖(AVC)後に出現する収縮後収縮(PSC)波(黄色矢印)である。
The marked PSC motion was confirmed by using strain imaging; it delays the two subsequent diastolic events, E_TDI and A_TDI waves.
顕著なPSC運動はストレインイメージングによって確認され、これにより後続する2つの拡張期イベントであるE_TDI波およびA_TDI波が遅延する。
E-G, Longitudinal systolic strain recordings using speckle tracking from the left apical 4-chamber view.
E-G、左心尖部四腔像からスペックルトラッキングを用いて記録した縦方向収縮期ストレイン。
E, Healthy cat.
E、健常猫。
All segments undergo systolic regional shortening; therefore, systolic strain is negative and homogeneously encoded red.
すべてのセグメントで収縮期局所短縮が認められるため、収縮期ストレインは負値となり、一様に赤色で表示される。
F, Cat with segmental IVSH.
F、区域性IVSHを有する猫。
Affected septal segments undergo abnormal lengthening in early systole (arrow) and are therefore encoded blue (left panel).
障害された中隔セグメントでは収縮早期に異常な延長(矢印)が認められるため、青色で表示される(左パネル)。
Right panel: 6 corresponding LV longitudinal strain vs. time curves, confirming abnormal positive strain for the 2 abnormal IVS segments (arrow).
右パネル:対応する6つの左室縦方向ストレイン対時間曲線であり、異常な2つのIVSセグメントにおける異常な陽性ストレインを確認できる(矢印)。
G, Cat with diffuse HCM.
G、びまん性HCMを有する猫。
PSC is present (yellow arrow), occurring during the diastolic phase.
拡張期にPSC(黄色矢印)が認められる。
All myocardial segments undergo an abnormal lengthening at early systole (yellow star).
すべての心筋セグメントで収縮早期に異常な延長(黄色星印)が認められる。
Ao, Aorta; AVO, aortic valve opening; LA, left atrium; LV, left ventricle.
Ao、大動脈;AVO、大動脈弁開放;LA、左心房;LV、左心室。
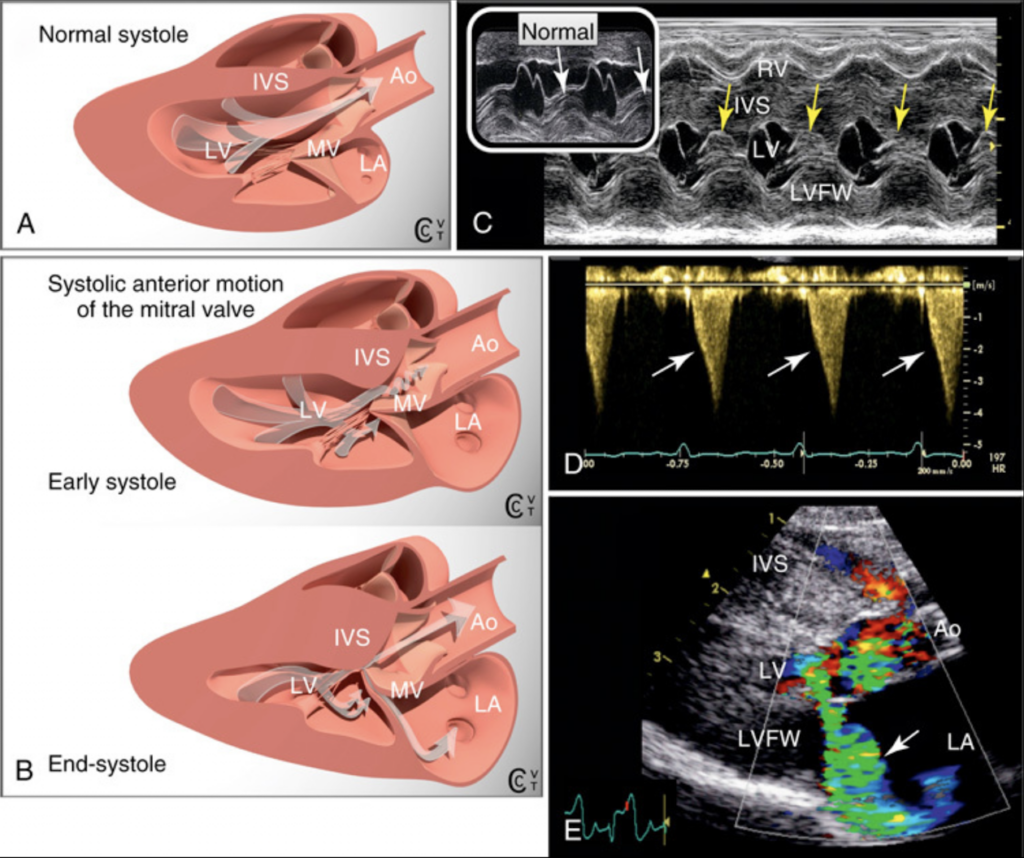
Systolic anterior motion of the mitral valve (MV) and obstructive hypertrophic cardiomyopathy.
僧帽弁(MV)の収縮期前方運動(SAM)と閉塞性肥大型心筋症。
A-B, In normal cats (A), the MV does not protrude into the left ventricular outflow tract (LVOT) during systole.
A-B、正常猫(A)では、収縮期にMVは左室流出路(LVOT)内へ突出しない。
B, With obstructive hypertrophic cardiomyopathy (OHCM), dynamic LVOT obstruction results from hypertrophy of the basal interventricular septum (IVS) and/or MV systolic anterior motion (SAM), which is an abnormal motion of the MV towards the LVOT in systole.
B、閉塞性肥大型心筋症(OHCM)では、動的LVOT閉塞は基部IVS肥大および/またはMVの収縮期前方運動(SAM)によって生じる。SAMとは、収縮期にMVがLVOT方向へ異常移動する現象である。
It causes mid- to late systolic contact between the MV and the IVS.
これにより、収縮中期から後期にかけてMVとIVSの接触が生じる。
The mechanism was long debated²⁹˒³⁵˒⁸¹ and is now considered to arise from systolic left ventricular (LV) flow pushing the underside of both MV leaflets towards the IVS, due to an abnormally ↑ “angle of attack” between direction of flow and MV leaflets in early systole.
その機序については長年議論されてきたが²⁹˒³⁵˒⁸¹、現在では、収縮早期における血流方向とMV弁尖との間の「迎角(angle of attack)」異常増大により、収縮期左室血流が両MV弁尖の下面をIVS方向へ押し出すことによると考えられている。
This greater angle of attack is due to (1) altered intra-LV flow direction (coming closer to the MV) due to the IVS bulge, and (2) altered MV geometry (MV leaflet protrusion and coaptation point closer to the IVS due to LV papillary muscle hypertrophy).⁸¹
この迎角増大は、(1)IVS膨隆による左室内血流方向の変化(MVにより近づく)、および(2)MV形態変化(左室乳頭筋肥大に伴うMV弁尖突出および接合点のIVS接近)による。⁸¹
In OHCM, SAM can affect the septal MV leaflet (41%), chordae tendineae (14%), or both (45%).
OHCMでは、SAMは中隔側MV弁尖(41%)、腱索(14%)、または両方(45%)に認められる。
Chordal SAM has been noted in healthy cats (16%) and cats with non-obstructive hypertrophic cardiomyopathy (56%) but MV SAM has not.²⁹
腱索SAMは健常猫(16%)および非閉塞性肥大型心筋症猫(56%)でも認められるが、MV SAMは認められない。²⁹
C, M-mode tracings showing MV SAM in a cat with OHCM (yellow arrows) but not in a normal cat.
C、OHCM猫ではMV SAM(黄色矢印)を示すMモード波形が認められるが、正常猫では認められない。
D, Continuous-wave Doppler recording in a cat with OHCM and SAM.
D、OHCMおよびSAMを有する猫における連続波ドプラ記録。
There is an ↑ peak systolic aortic velocity (4 m/s; normal <2 m/s)⁸⁸ and a late-peaking flow profile, characterized by an asymmetric, concave waveform owing to sudden flow acceleration at mid-systole (arrows).
収縮期大動脈最大流速上昇(4 m/s;正常 <2 m/s)⁸⁸および、収縮中期での急激な血流加速(矢印)により非対称かつ凹型波形を呈する遅峰性血流プロファイルが認められる。
This confirms dynamic LVOT obstruction (moderate: 64 mm Hg LVOT-Ao pressure gradient).
これは動的LVOT閉塞を示している(中等度:LVOT-Ao圧較差64 mmHg)。
E, (same cat as in C): double systolic turbulent jet on color-flow Doppler, as commonly observed with MV SAM.
E、(Cと同一症例):MV SAMで一般的に観察される、カラードプラ上の二重収縮期乱流ジェット。
Typically, there is aliased ejection flow in the narrowed LVOT, and a simultaneous mitral regurgitation jet that hugs the posterior LA wall.
典型的には、狭窄したLVOT内にエイリアシングを伴う駆出血流と、左心房(LA)後壁に沿う僧帽弁逆流ジェットが同時に認められる。
Ao, aorta; LA, left atrium; LV, left ventricle; LVFW, left ventricular free wall; RV, right ventricle.
Ao、大動脈;LA、左心房;LV、左心室;LVFW、左室自由壁;RV、右心室。
Reproduced from Chetboul V and Taton C, editors. Encyclopédie d’imagerie cardiovasculaire ultrasonore du chien et du chat. Issy-les-Moulineaux: 772 pp 2018 Elsevier Masson SAS. All rights reserved.
Chetboul VおよびTaton C編『Encyclopédie d’imagerie cardiovasculaire ultrasonore du chien et du chat』より転載。Issy-les-Moulineaux、772頁、2018年、Elsevier Masson SAS。無断転載禁止。
Clinical Presentation at Diagnosis:診断時の臨床症状
Clinical Signs:臨床徴候
Many cats with HCM show no overt clinical signs at the time of diagnosis (33-77%).³⁹˒⁴⁴˒⁴⁵˒⁶⁸˒⁸² These cats are usually referred because of an abnormal cardiac auscultation on routine examination, for screening purposes before mating, or for cardiovascular evaluation before anesthesia. Most cats that show clinical manifestations due to HCM (70-80%) have signs of CHF, i.e., mainly tachypnea and dyspnea related to pulmonary edema and/or pleural effusion (reported in 18-46% of HCM cats at presentation).³⁹˒⁴⁴˒⁴⁵˒⁸² Coughing is reported more rarely than in dogs. Ascites related to right-sided CHF is rare.³⁹ Anorexia and lethargy are common in cats with CHF and can even precede the onset of other signs of CHF by 24-72 hours. An antecedent event that may have precipitated decompensation is reported in 14-50% of cases, 7-15 days prior to the onset of signs of CHF. These include intravenous (IV) fluid therapy, general anesthesia, surgery, corticosteroid administration, and trauma.³⁹˒⁴⁴
HCM猫の多くは、診断時に明らかな臨床徴候を示さない(33〜77%)。³⁹˒⁴⁴˒⁴⁵˒⁶⁸˒⁸² これらの猫は通常、定期検査時の異常心音、交配前スクリーニング、あるいは麻酔前心血管評価を契機として紹介される。HCMに起因する臨床症状を示す猫(70〜80%)の大多数では、CHF徴候が認められ、主として肺水腫および/または胸水に関連した頻呼吸および呼吸困難を呈する(初診時HCM猫の18〜46%で報告)。³⁹˒⁴⁴˒⁴⁵˒⁸² 咳は犬よりまれである。右心性CHFに関連した腹水もまれである。³⁹食欲不振および嗜眠はCHF猫で一般的であり、他のCHF徴候に先行して24〜72時間前から出現する場合もある。代償不全を誘発した可能性のある先行イベントは、CHF徴候発現の7〜15日前に、14〜50%の症例で報告されている。これには、静脈内輸液療法、全身麻酔、外科手術、コルチコステロイド投与、および外傷が含まれる。³⁹˒⁴⁴
The second most common clinical signs are related to ATE, detected in 4-17% of cats with HCM at the time of diagnosis with or without concomitant CHF. Signs mainly are characterized by acute bilateral and painful hindlimb paresis, and less commonly forelimb paresis (ch. 238).³⁹˒⁴⁴˒⁴⁵˒⁶⁸ Other clinical signs can include syncope and weakness; they are observed in 1-6% of cats with HCM at diagnosis.³⁹˒⁴⁴˒⁶⁸ Laboured, open-mouth breathing despite the absence of radiographic and echocardiographic signs of CHF is reported in cats with HCM.⁴⁵ One possible explanation is that these cats are suffering from angina-like chest pain, similar to that which is experienced by human patients with HCM.⁴⁵ Lastly, some cats with HCM can die unexpectedly, with no premonitory clinical signs.⁸³
次に多い臨床徴候はATE関連であり、CHF併発の有無を問わず、診断時HCM猫の4〜17%で認められる。徴候は主として、急性両側性で疼痛を伴う後肢不全麻痺であり、前肢不全麻痺はよりまれである(第238章)。³⁹˒⁴⁴˒⁴⁵˒⁶⁸その他の臨床徴候として、失神および虚弱があり、診断時HCM猫の1〜6%で認められる。³⁹˒⁴⁴˒⁶⁸HCM猫では、X線検査および心エコー検査上CHF所見が存在しないにもかかわらず、努力性開口呼吸が認められる場合がある。⁴⁵ その一因として、ヒトHCM患者でみられるものと類似した狭心症様胸痛をこれらの猫が経験している可能性が挙げられている。⁴⁵最後に、一部のHCM猫では、前駆症状なく突然死する場合がある。⁸³
Cardiac Auscultation:心臓聴診
Cardiac auscultation is abnormal in most reported cats with HCM (78-92%).³⁹˒⁴⁴˒⁴⁵ The most common abnormality is a parasternal systolic heart murmur (64-89% of HCM cats), heard best over the left apex or cranially and resulting from MV regurgitation and LVOTO, respectively (ch. 38).³⁹˒⁴⁴ These murmurs are often dynamic, meaning of variable grade and increasing with heart rate. They are found more commonly in cats without clinical signs (89-92%) than in those showing clinical signs (77%).³⁹˒⁴⁵ This may be explained by the fact that incidentally-detected heart murmurs are one of the main reasons that veterinarians refer cats for echocardiograms. A gallop sound (ch. 38) and arrhythmias (ch. 230) are detected in up to 33% and 6-10% of cats with HCM, respectively.³⁹˒⁴⁴˒⁴⁵ Unlike heart murmurs, both are uncommon in cats with subclinical HCM (<10% and ≤5%, respectively), probably because they reflect severe myocardial lesions.³⁹˒⁴⁵
HCM猫の大多数では、心臓聴診異常が認められる(78〜92%)。³⁹˒⁴⁴˒⁴⁵ 最も一般的な異常は胸骨傍収縮期心雑音であり(HCM猫の64〜89%)、左心尖部またはより頭側で最も明瞭に聴取され、それぞれMV逆流およびLVOTOに起因する(第38章)。³⁹˒⁴⁴これらの雑音はしばしば動的であり、すなわち強度が変動し、心拍数増加に伴って増強する。これらは臨床徴候を示す猫(77%)よりも、無症候猫(89〜92%)でより高頻度に認められる。³⁹˒⁴⁵ これは、偶発的に発見された心雑音が、獣医師が猫を心エコー検査へ紹介する主要理由の1つであることによって説明される可能性がある。奔馬調律(第38章)および不整脈(第230章)は、それぞれ最大33%および6〜10%のHCM猫で検出される。³⁹˒⁴⁴˒⁴⁵心雑音とは異なり、これらはいずれも無症候性HCM猫ではまれであり(それぞれ<10%および≤5%)、おそらく重度心筋病変を反映しているためと考えられる。³⁹˒⁴⁵
Electrocardiographic Findings:心電図所見
Various nonspecific morphological electrocardiographic (ECG, ch. 96) alterations are associated with feline HCM, resulting from LVH (QRS amplitude >0.9 mV) and LAE (P wave duration >40 ms, PR interval >90 ms).¹˒⁸⁴ The latter P wave-related ECG indices have a low sensitivity (12-60%) but high specificity (81-100%) for predicting LAE in cats with cardiomyopathy.⁸⁴ A left axis deviation suggestive of left anterior fascicular block is reported in 11-33% of HCM cats, more commonly than in those suffering from other cardiomyopathies.¹ Arrhythmias also are frequently noted (approximately one-third of cats with HCM in one report; premature ventricular complexes in 65% of these).⁶⁸˒⁸⁵ Myocardial diseases, predominantly HCM, represent the most common cause of ventricular arrhythmias in cats.⁸⁶ Other arrhythmias include supraventricular premature complexes, atrioventricular (AV) blocks or AV dissociation (1%), and atrial fibrillation (AF, 0.5%).¹˒³⁹˒⁶⁸ Use of 24-hour Holter monitoring (ch. 96), which is more sensitive than “in-clinic ECG” for arrhythmia detection, shows that cats with both compensated and decompensated HCM have more frequent and complex ventricular and supraventricular arrhythmias than normal cats.⁸⁵˒⁸⁷ In one study,⁸⁵ all cats with subclinical HCM had ventricular arrhythmias, with 82% exhibiting complex arrhythmias vs. 20% for normal cats despite similar heart rate; 87% had supraventricular arrhythmias with 23% exhibiting complexity, as compared to 60% and 13%, respectively, for normal cats. Whether such arrhythmias are associated with an increased risk of sudden cardiac death or a shorter life span requires further investigation.
さまざまな非特異的形態学的心電図(ECG、第96章)異常が猫HCMに関連して認められ、LVH(QRS振幅 >0.9 mV)およびLAE(P波持続時間 >40 ms、PR間隔 >90 ms)に起因する。¹˒⁸⁴後者のP波関連ECG指標は、心筋症猫におけるLAE予測に対して感度は低い(12〜60%)が、特異度は高い(81〜100%)。⁸⁴左前枝ブロックを示唆する左軸偏位は、他の心筋症より高頻度に、HCM猫の11〜33%で報告されている。¹不整脈も頻繁に認められ(ある報告ではHCM猫の約3分の1)、そのうち65%で心室性期外収縮が認められた。⁶⁸˒⁸⁵心筋疾患、特にHCMは、猫における心室性不整脈の最も一般的な原因である。⁸⁶その他の不整脈として、上室性期外収縮、房室(AV)ブロックまたはAV解離(1%)、および心房細動(AF、0.5%)が含まれる。¹˒³⁹˒⁶⁸24時間ホルターモニタリング(第96章)は、不整脈検出において「院内ECG」より高感度であり、代償性および非代償性HCM猫では、正常猫よりも高頻度かつ複雑な心室性・上室性不整脈が認められることを示している。⁸⁵˒⁸⁷ある研究では、⁸⁵ 無症候性HCM猫のすべてに心室性不整脈が認められ、その82%で複雑性不整脈を呈していたのに対し、正常猫では20%であった。心拍数は同等であったにもかかわらず、この差が認められた。また、87%で上室性不整脈が認められ、その23%が複雑性を示したのに対し、正常猫ではそれぞれ60%および13%であった。このような不整脈が突然心臓死リスク増加あるいは寿命短縮と関連するかどうかについては、さらなる検討が必要である。
Clinical Course and Prognosis:臨床経過および予後
Survival times for cats with HCM are highly variable. Some live years, have a normal life expectancy, and die from non-cardiac causes, whereas others die several days after the diagnosis is made or even die suddenly before an antemortem diagnosis of HCM can be established. For example, an overall median survival time of 709 days with a wide range (2-4418 days) was reported for HCM cats that survived >24 hours after the diagnosis was made.⁴⁴ This highly variable survival time was also shown in another study (median, 1276 days; range, 0-3617 days).⁴⁵ Cardiac deaths related to HCM mainly include spontaneous deaths or euthanasia either secondary to ATE or CHF (each representing ~33-50% of all cardiac deaths), and also sudden death (10-25% of all HCM-related deaths).³⁹˒⁴⁴˒⁶⁸˒⁸² Various clinical, breed, genetic and imaging risk factors associated with cardiac death have been identified³⁹˒⁴⁴˒⁴⁵˒⁵⁸˒⁶⁸:
HCM猫の生存期間は極めて多様である。長年生存し、正常寿命を全うし、非心疾患で死亡する猫もいれば、診断後数日以内に死亡する猫や、生前診断が確立される前に突然死する猫も存在する。例えば、診断後24時間以上生存したHCM猫では、全体中央値生存期間709日(範囲2〜4418日)が報告されている。⁴⁴ この高度な生存期間変動は、別研究(中央値1276日、範囲0〜3617日)でも確認されている。⁴⁵HCM関連心臓死には、主としてATEまたはCHFに続発する自然死あるいは安楽死(それぞれ全心臓死の約33〜50%)に加え、突然死(全HCM関連死亡の10〜25%)が含まれる。³⁹˒⁴⁴˒⁶⁸˒⁸²心臓死に関連するさまざまな臨床的、品種的、遺伝学的、および画像診断学的危険因子が同定されている。³⁹˒⁴⁴˒⁴⁵˒⁵⁸˒⁶⁸
Clinical Signs:臨床徴候
The reported percentage of HCM cats dying for cardiac reasons varies from 37% to 81%, depending on the presence or absence of clinical signs at diagnosis.²¹˒³⁹˒⁴⁴˒⁴⁵˒⁶⁸ Much longer survival times have been reported for cats with subclinical HCM than in those showing clinical signs. In the latter, wide ranges of life spans exist within each clinical status category.³⁹˒⁴⁴˒⁴⁵˒⁸² In 260 cats with HCM, those with occult HCM lived the longest (median, 1129 days), followed by cats presenting with syncope (654 days), CHF (563 days), and ATE (184 days).⁴⁴ Another study of 127 cats with HCM showed that those without CHF survived longer (median >3617 days) than those with CHF (median, 194 days).⁴⁵ In a third study, 80% of cats with subclinical HCM died of non-cardiac causes, whereas 80% of cats with overt clinical signs caused by HCM died of cardiac causes.³⁹ Other negative clinical predictors of cardiac death include age, and presence of a gallop sound and arrhythmias at diagnosis. Thus, in cats with subclinical cardiomyopathy, gallop sounds and arrhythmias are considered as risk factors for imminent CHF and ATE, which explains why they are among the criteria for stage B2 according to the ACVIM feline cardiomyopathy staging system (Table 234.2).³˒⁶⁸
心臓関連死を示すHCM猫の割合は、診断時臨床徴候の有無により37〜81%と変動する。²¹˒³⁹˒⁴⁴˒⁴⁵˒⁶⁸無症候性HCM猫では、臨床徴候を示す猫より著しく長い生存期間が報告されている。一方、症候性群では、各臨床カテゴリー内で寿命幅が大きい。³⁹˒⁴⁴˒⁴⁵˒⁸²260頭のHCM猫を対象とした研究では、潜在性HCM群が最長生存(中央値1129日)を示し、続いて失神群(654日)、CHF群(563日)、ATE群(184日)であった。⁴⁴別の127頭研究では、CHFを伴わない群の生存期間(中央値 >3617日)は、CHF群(中央値194日)より長かった。⁴⁵さらに別研究では、無症候性HCM猫の80%は非心疾患で死亡した一方、HCMに起因する明らかな臨床徴候を示した猫の80%は心疾患関連死であった。³⁹その他の負の予後因子として、年齢、診断時の奔馬調律および不整脈の存在が含まれる。したがって、無症候性心筋症猫では、奔馬調律および不整脈は差し迫ったCHFおよびATEの危険因子とみなされ、これがACVIM猫心筋症病期分類システムにおけるB2ステージ基準に含まれている理由である(表234.2)。³˒⁶⁸
Breed:品種
Ragdolls have shorter survival times than other cats (median survival, 19 days vs. 1297 days respectively).⁴⁵ In one study without Ragdolls, the age at first cardiac event (CHF, ATE, syncope, sudden death) was lower in Maine Coon cats (median age, 2.5 years) than in other cats (7.0 years), with half of the Maine Coon deaths attributed to cardiac causes whereas most (>75%) deaths of Chartreux and Persian cats were attributed to non-cardiac causes.³⁹
ラグドールは他品種より生存期間が短い(中央値19日対1297日)。⁴⁵ラグドールを除外したある研究では、初回心イベント(CHF、ATE、失神、突然死)発生年齢は、メインクーンで他品種より若齢であった(中央値2.5歳対7.0歳)。また、メインクーン死亡例の半数は心臓原因であった一方、シャルトリューおよびペルシャでは死亡の大多数(>75%)が非心臓原因であった。³⁹
Genetic Status:遺伝学的状態
Ragdoll cats that are homozygous for the MyBPC3 R820W mutation are more likely to die from cardiac death and have a shorter time to cardiac death than heterozygous and wild-type cats (median age at cardiac death, 5.7 years vs. >16.7 years and >15.2 years, respectively).⁵⁸
MyBPC3 R820W変異ホモ接合体ラグドールは、ヘテロ接合体および野生型猫より、心臓死しやすく、心臓死までの期間も短い(心臓死中央値年齢:5.7歳対>16.7歳および>15.2歳)。⁵⁸
Imaging Variables:画像診断変数
LAE, assessed using several methods,⁷⁴˒⁸⁸ is consistently negatively associated with survival time in both subclinical and overt HCM.²¹˒⁴⁴˒⁴⁵˒⁶⁸˒⁷⁰ In cats with HCM, the median survival time is much longer (>3617 days) when LA size is normal than when there is LAE (229 days).⁴⁵ Other imaging predictors of increased risk of cardiac death include severe LVH (wall thickness ≥9.0 mm), decreased systolic function (LV fractional shortening [FS%] ≤30%), decreased LA function (assessed by LA FS%), RV enlargement, regional wall hypokinesis, spontaneous echo contrast/thrombus or both, and a restrictive diastolic filling pattern.²¹˒⁴⁴˒⁴⁵˒⁶⁸˒⁸⁹ In cats with subclinical cardiomyopathy, most of these imaging predictors, together with gallop sounds and arrhythmias, are considered as risk factors for imminent CHF and ATE, which explains why they are used for defining ACVIM stage B2 (Table 234.2).³ Interestingly, unlike in people, dynamic LVOTO is not known to be associated with a worse prognosis: no statistically significant differences have been found between cats with OHCM and those with non-obstructive HCM for cardiovascular morbidity or mortality, time from diagnosis to development of morbidity, or cardiovascular survival.⁹⁰
複数方法で評価されたLAEは、⁷⁴˒⁸⁸ 無症候性および症候性HCMの双方において、生存期間と一貫して負の関連を示す。²¹˒⁴⁴˒⁴⁵˒⁶⁸˒⁷⁰
HCM猫では、LAサイズ正常時の中央値生存期間(>3617日)は、LAE存在時(229日)より著しく長い。⁴⁵
その他の心臓死リスク増加を示す画像診断学的予測因子として、重度LVH(壁厚 ≥9.0 mm)、収縮機能低下(左室短縮率[FS%] ≤30%)、LA機能低下(LA FS%で評価)、RV拡大、局所壁運動低下、自発性エコーコントラスト/血栓、あるいはその両方、および拘束性拡張流入パターンが挙げられる。²¹˒⁴⁴˒⁴⁵˒⁶⁸˒⁸⁹
無症候性心筋症猫では、これら画像診断学的予測因子の多くに加え、奔馬調律および不整脈も、差し迫ったCHFおよびATEの危険因子とみなされる。このため、それらはACVIM B2ステージ定義に使用されている(表234.2)。³
興味深いことに、ヒトとは異なり、動的LVOTOは予後悪化と関連しないと考えられている。OHCM猫と非閉塞性HCM猫の間で、心血管罹患率、死亡率、診断から罹患発症までの期間、あるいは心血管生存率に統計学的有意差は認められていない。⁹⁰
RESTRICTIVE CARDIOMYOPATHY:拘束型心筋症
Definition—Pathological Lesions:定義—病理学的病変
Human RCM:ヒトのRCM
Human RCM is an uncommon heart muscle disease primarily characterized by impaired ventricular filling due to increased myocardial stiffness or reduced compliance of either or both ventricles (mainly LV), with normal or near-normal systolic function and wall thicknesses.⁷˒⁹¹⁻⁹⁴ The reduced ventricular compliance restricts ventricular filling (hence the term “restrictive”), with secondary increased end-diastolic ventricular filling pressure. This results in marked LA or biatrial enlargement. In the early stages, global systolic function is normal, and then altered systolic function is usually observed as the disease progresses.¹¹˒⁹⁴ Human RCM represents a heterogeneous group of heart disorders subdivided into primary and secondary RCM.¹¹˒⁹³˒⁹⁴ Causes of secondary RCM include infiltrative diseases (e.g., amyloidosis, sarcoidosis, Gaucher and Hurler diseases) and storage diseases (e.g., hemochromatosis, glycogen storage disorders, and Fabry disease). Secondary RCM, especially endomyocardial fibrosis, is also reported in the hypereosinophilic syndrome and as an iatrogenic complication (radiation, drugs).⁹¹˒⁹⁴ Primary human RCM is characterized by patchy to diffuse interstitial myocardial fibrosis with possible fibrosis of the sinoatrial and AV nodes, resulting in AV blocks.⁹¹ Endomyocardial fibrosis is a specific form of primary RCM, characterized by marked endocardial fibrosis in addition to myocardial fibrosis.⁹⁵˒⁹⁶ Similarly to HCM, familial forms of primary RCM are reported, with most identified genes encoding for sarcomere or Z-disk proteins, e.g., cardiac troponin genes and MYH7.⁹⁷⁻⁹⁹ Interestingly, in addition to these genetic similarities, “overlap” or “crossover” phenotypes of RCM and HCM have been observed in families with mutations in sarcomeric genes, suggesting that some RCM cases may be considered as “minimally hypertrophic” HCM phenotypes.⁹⁴
ヒトの拘束型心筋症(RCM)は比較的まれな心筋疾患であり、主として心筋の硬化あるいは一方または両方の心室(主に左心室)のコンプライアンス低下による心室充満障害を特徴とする。収縮機能および壁厚は正常またはほぼ正常である。⁷˒⁹¹⁻⁹⁴ 心室コンプライアンスの低下により心室充満が制限され(“restrictive”の語源)、二次的に拡張末期心室充満圧が上昇する。その結果、著明な左心房または両心房拡大が生じる。初期段階では全体的な収縮機能は正常であるが、疾患進行に伴い収縮機能障害が通常認められるようになる。¹¹˒⁹⁴ ヒトRCMは異質性の高い心疾患群であり、原発性RCMと続発性RCMに分類される。¹¹˒⁹³˒⁹⁴ 続発性RCMの原因には浸潤性疾患(例:アミロイドーシス、サルコイドーシス、ゴーシェ病、ハーラー病)および蓄積病(例:ヘモクロマトーシス、糖原病、Fabry病)が含まれる。続発性RCM、特に心内膜心筋線維症は、好酸球増加症候群や医原性合併症(放射線、薬剤)としても報告されている。⁹¹˒⁹⁴ 原発性ヒトRCMは、斑状からびまん性の間質性心筋線維症を特徴とし、洞房結節および房室結節の線維化を伴うことがあり、その結果として房室ブロックを生じる。⁹¹ 心内膜心筋線維症は原発性RCMの特殊型であり、心筋線維症に加えて著明な心内膜線維症を特徴とする。⁹⁵˒⁹⁶ HCMと同様に、原発性RCMにも家族性症例が報告されており、同定された遺伝子の多くはサルコメア蛋白またはZ帯蛋白をコードするものである。例えば心筋トロポニン遺伝子やMYH7などが含まれる。⁹⁷⁻⁹⁹ 興味深いことに、これらの遺伝学的類似性に加え、サルコメア遺伝子変異を有する家系においてRCMとHCMの“オーバーラップ”あるいは“クロスオーバー”表現型が観察されており、一部のRCM症例は“最小限の肥大型”HCM表現型とみなせる可能性が示唆されている。⁹⁴
Feline RCM:猫のRCM
Similar to human forms of primary RCM, “myocardial RCM” and “endomyocardial fibrosis RCM” have been identified in the cat.¹˒¹⁶˒¹⁷˒¹⁰⁰⁻¹⁰⁴ There is a greater frequency in cats than what is reported in humans, as RCM is currently the second most common feline primary cardiomyopathy (Figure 234.9).²² In one study of 92 cats with RCM, the most common form was myocardial RCM by far (90% of cases).¹⁰¹ At the time of this writing, no causal mutations for either feline RCM forms have been identified. Nevertheless and interestingly, histopathological features of feline HCM (e.g., myocyte disarray, abnormal intramural coronary arterioles, patchy replacement scarring) are found in most cats with RCM, thus suggesting that feline RCM could be the phenotypic expression of sarcomere mutations.¹⁷ The hallmark feature of feline endomyocardial fibrosis is a prominent endomyocardial scar commonly appearing as a distinct “tubular” lesion bridging the IVS and LVFW that may result in mid- to apical intracavitary stenosis (Figure 234.9, B; Video 234.12).¹⁶ The less common form, feline endomyocardial fibrosis, is characterized by diffuse endomyocardial scar resulting in reduction or obliteration of the LV cavity (Figure 234.9, A).¹⁶ In both endomyocardial forms, endocardial thickening may also involve atrial chambers, the RV (rarely), or both, in association with myocardial interstitial fibrosis, various degrees of myocyte hypertrophy and necrosis, intramural coronary arteriosclerosis and inflammatory infiltrates.¹⁶ Such inflammatory infiltrates are also described in the feline “myocardial RCM” form, suggesting a possible role of viral infection and/or immune-mediated lesions.¹⁰⁵ In one report, interstitial pneumonia was found in >25% of cats with RCM; the authors questioned whether the same agent or process could affect both the heart and lungs.¹⁰⁰ More recently, some investigators have suggested that Bartonella spp. may play a primary role or act as a cofactor in the pathogenesis of endomyocarditis-LV endocardial fibrosis.¹⁰⁶
ヒト原発性RCMと同様に、「心筋型RCM」および「心内膜心筋線維症型RCM」が猫でも同定されている。¹˒¹⁶˒¹⁷˒¹⁰⁰⁻¹⁰⁴ 猫ではヒトより高頻度に認められ、RCMは現在、猫において2番目に多い原発性心筋症である(図234.9)。²² 92例のRCM猫を対象とした研究では、最も一般的な病型は圧倒的に心筋型RCMであり(90%)、¹⁰¹ 本稿執筆時点では、いずれの猫RCM病型についても原因遺伝子変異は同定されていない。しかし興味深いことに、猫HCMの組織病理学的特徴(例:心筋細胞錯綜配列、壁内冠動脈細動脈異常、斑状置換性瘢痕化)がRCM猫の大部分で認められ、猫RCMがサルコメア変異の表現型である可能性が示唆されている。¹⁷ 猫心内膜心筋線維症の特徴的病変は、IVSとLVFWを橋渡しする明瞭な“管状”病変として現れる顕著な心内膜瘢痕であり、左室中部から心尖部にかけての心室内狭窄を引き起こす場合がある(図234.9, B;Video 234.12)。¹⁶ よりまれな型である猫心内膜心筋線維症では、びまん性心内膜瘢痕によって左室腔の縮小または閉塞が生じる(図234.9, A)。¹⁶ 両方の心内膜型において、心内膜肥厚は心房腔、まれには右心室、またはその両方にも及ぶことがあり、心筋間質線維症、種々の程度の心筋細胞肥大および壊死、壁内冠動脈硬化症、炎症性浸潤を伴う。¹⁶ このような炎症性浸潤は猫の「心筋型RCM」においても記載されており、ウイルス感染および/または免疫介在性病変の関与が示唆されている。¹⁰⁵ ある報告では、RCM猫の25%以上で間質性肺炎が認められ、著者らは同一の病因または病態が心臓と肺の両方に影響を及ぼす可能性を指摘している。¹⁰⁰ さらに近年、一部の研究者はBartonella属菌が心内膜炎―左室心内膜線維症の病因において主要な役割を果たす、あるいは補助因子として作用する可能性を示唆している。¹⁰⁶
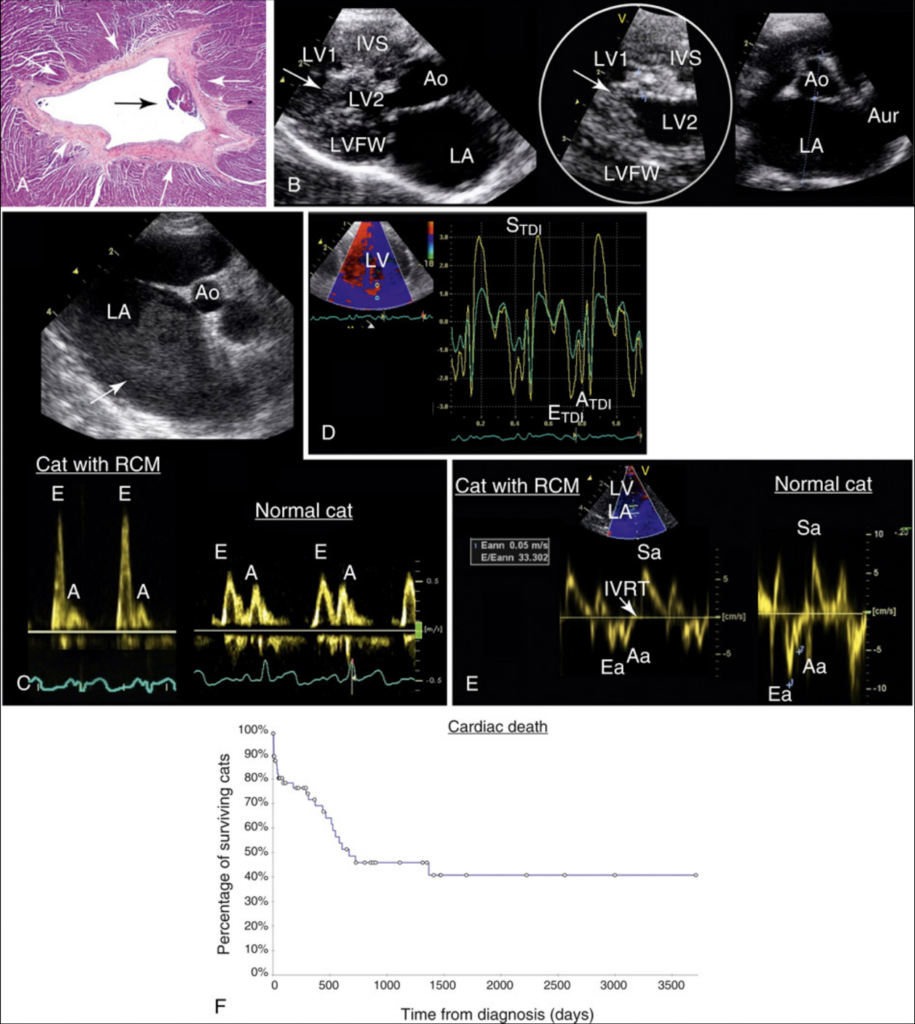
Representative findings in cats with restrictive cardiomyopathy.
拘束型心筋症猫における代表的所見。
A, Histologic evaluation of a left ventricular (LV) cross-sectional specimen from a cat with endomyocardial fibrosis that died suddenly.
A、突然死した心内膜心筋線維症猫の左室(LV)横断標本の組織学的評価。
There is a thick, circumferential LV endocardial scar (white arrows) and a mural thrombus (black arrow).
肥厚した全周性左室心内膜瘢痕(白矢印)および壁在血栓(黒矢印)が認められる。
Hematoxylin-eosin-saffron stain.
ヘマトキシリン・エオジン・サフラン染色。
B, Echocardiographic images from a cat with endomyocardial fibrosis.
B、心内膜心筋線維症猫の心エコー画像。
Left: a large heterogeneous bridging scar (arrow) connects the interventricular septum (IVS) and the left ventricular free wall (LVFW), dividing the LV cavity into apical (LV1) and basal (LV2) parts.
左:大きな不均一性架橋瘢痕(矢印)がIVSとLVFWを連結し、LV腔を心尖部(LV1)と基部(LV2)に分割している。
There is secondary left atrial (LA) dilation compared to the aorta (Ao).
Aoと比較して二次性LA拡大が認められる。
Middle: zoomed view of the bridging scar (arrow) with focal hyperechoic areas consistent with fibrosis.
中央:線維化に一致する局所的高エコー領域を伴う架橋瘢痕(矢印)の拡大像。
Right: marked auricular (Aur) and LA enlargement (end-diastolic LA:Ao ratio = 2.2; reference interval, 0.5-1.2).⁸⁸
右:著明な心耳(Aur)およびLA拡大(拡張末期LA:Ao比 = 2.2;基準範囲 0.5–1.2)。⁸⁸
C, Echocardiographic features of restrictive cardiomyopathy (RCM) in a cat.
C、猫における拘束型心筋症(RCM)の心エコー所見。
Top: smoke-like spontaneous echocontrast (arrow) indicative of blood stasis in the severely enlarged left atrium.
上段:高度拡大した左心房内の血流停滞を示唆する煙状自然エコーコントラスト(矢印)。
Bottom: compared to a normal cat (right), a cat with RCM (left) has a typical restrictive filling pattern: ↑ E:A (>2)⁷⁴ from both ↑ LA pressure and ↓ ventricular compliance with secondary ↑ LV diastolic pressure.
下段:正常猫(右)と比較して、RCM猫(左)では典型的拘束型充満パターンを示し、LA圧上昇および心室コンプライアンス低下に伴う二次性LV拡張期圧上昇により、E:A比上昇(>2)⁷⁴が認められる。
Decreased LA function may also contribute to the small A wave amplitude.
LA機能低下もA波振幅低下に寄与している可能性がある。
The E-wave deceleration time (30 ms) in the cat with RCM is short (30 ms; 92 ms for the normal cat; reference interval, 54-192 ms),¹⁷ due to rapid equalization of LA and LV pressures after early diastolic filling.
RCM猫におけるE波減速時間(30 ms)は短縮しており(正常猫92 ms;基準範囲54–192 ms)¹⁷、これは拡張早期充満後のLA圧とLV圧の急速な均衡化による。
D, Radial diastolic dysfunction in a cat with RCM using two-dimensional color tissue Doppler imaging (TDI) (right parasternal short axis view).
D、二次元カラー組織ドプライメージング(TDI)(右傍胸骨短軸像)を用いたRCM猫の放射方向拡張機能障害。
The subendocardial (yellow) and subepicardial (green) radial velocity profiles recorded with color TDI show low diastolic waves, especially in the subendocardium (E_TDI wave, 2.6 cm/s; reference interval, 5.7 ± 1.5 cm/s [3.5-10.8]).⁸⁸
カラーTDIで記録された心内膜下(黄色)および心外膜下(緑色)の放射方向速度プロファイルでは、特に心内膜下において低い拡張期波が認められる(E_TDI波、2.6 cm/s;基準範囲 5.7 ± 1.5 cm/s[3.5–10.8])。⁸⁸
E, Pulsed-wave TDI recording, lateral mitral valve (MV) annulus, in a cat with RCM (left).
E、RCM猫(左)における側方MV弁輪部のパルス波TDI記録。
Markedly ↓ diastolic velocities (Ea and Aa, cm/s), reflecting ↓ velocities of longitudinal diastolic motion: peak annular velocity during early diastole (Ea) = 5 cm/s (versus 9.8 cm/s for the normal cat; reference interval, >6 cm/s).⁷⁴
縦方向拡張運動速度低下を反映して、著明な拡張期速度低下(EaおよびAa、cm/s)が認められる。拡張早期最大弁輪速度(Ea)は5 cm/sであり(正常猫9.8 cm/s;基準範囲 >6 cm/s)。⁷⁴
Additionally, in the cat with RCM, the peak MV E wave velocity was 1.66 m/s, producing an E:Ea = 33 (6.6 in the normal cat; reference interval, <12).⁷⁴
さらに、RCM猫ではMV E波最大速度が1.66 m/sであり、E:Ea比は33であった(正常猫では6.6;基準範囲 <12)。⁷⁴
By combining peak MV E wave velocity (mainly determined by LV filling pressure and relaxation) with Ea (mainly depends on relaxation) the E:Ea ratio is an index reflecting LV filling pressure (as the effect of relaxation on E is minimized).⁷⁴
MV E波最大速度(主にLV充満圧および弛緩に依存)とEa(主に弛緩に依存)を組み合わせることで得られるE:Ea比は、LV充満圧を反映する指標となる(Eに対する弛緩の影響が最小化されるため)。⁷⁴
F, Kaplan-Meier curve illustrating survival time in 69 cats with RCM (myocardial form), excluding cats that died <24 hours after diagnosis.
F、診断後24時間以内に死亡した症例を除外した、RCM(心筋型)猫69頭における生存期間を示すKaplan-Meier曲線。
Median (range) survival time from diagnosis was 667 (2-3710) days.
診断からの生存期間中央値(範囲)は667日(2–3710日)であった。
Considering all-cause death, median survival time was 436 days.
全死亡原因を含めた場合、生存期間中央値は436日であった。
Circles denote censored observations.¹⁰¹
丸印は打ち切り症例を示す。¹⁰¹
Aa, Sa, Peak annular velocities during late diastole and systole, respectively; A_TDI, peak myocardial velocity during late diastole; E_TDI, peak myocardial velocity during early diastole; S_TDI, peak myocardial velocity during systole.
Aa、Sa、それぞれ拡張後期および収縮期の最大弁輪速度;A_TDI、拡張後期最大心筋速度;E_TDI、拡張早期最大心筋速度;S_TDI、収縮期最大心筋速度。
A, Courtesy Prof. Jean-Jacques Fontaine, Pathology Department, National Veterinary School of Alfort, France.
A、フランス・アルフォール国立獣医学校病理学教室 Jean-Jacques Fontaine教授提供。
Epidemiology—Clinical Presentation at Diagnosis:疫学—診断時の臨床像
In a report of 35 cats with RCM, the mean age at diagnosis was 10 ± 4 years with a wide range (1.5-17.1).¹⁷ Similarly, in another study of 92 cats with RCM, the median age at diagnosis was 8.6 years (interquartile range = 4.1-12.4), with males (49%) and females (51%) equally represented.¹⁰¹ Conversely, most affected cats were males (59-71%) in other reports.¹⁷˒¹⁰³˒¹⁰⁴ Cats of various breeds can develop RCM (e.g., Burmese, Siamese, Persian, Birman, Maine Coon, Norwegian Forest Cat), with a predominance of DSH cats (67-71%), but no familial link has been reported.¹⁷˒¹⁰³˒¹⁰⁴
35例のRCM猫を対象とした報告では、診断時平均年齢は10 ± 4歳であり、範囲は1.5〜17.1歳と広範囲であった。¹⁷ 同様に、92例のRCM猫を対象とした別の研究では、診断時年齢中央値は8.6歳(四分位範囲4.1〜12.4歳)であり、雄(49%)と雌(51%)はほぼ同数であった。¹⁰¹ 一方、別の報告では罹患猫の多くが雄(59〜71%)であった。¹⁷˒¹⁰³˒¹⁰⁴ RCMはさまざまな猫種(例:バーミーズ、シャム、ペルシャ、バーマン、メインクーン、ノルウェージャンフォレストキャット)で発症しうるが、DSHが優勢(67〜71%)であり、家族性関連は報告されていない。¹⁷˒¹⁰³˒¹⁰⁴
Almost all cats with RCM show clinical signs at the time of diagnosis, predominantly related to CHF.¹⁷˒²¹˒²²˒¹⁰¹˒¹⁰⁴ In the report on 35 cats with RCM, 91% presented with CHF, 6% with lethargy and 3% with syncope and transient paresis.¹⁷ Similarly, in the study of 92 cats with RCM, 70% had at least 1 clinical sign related to RCM at the time of diagnosis.¹⁰¹ The most common sign was dyspnea related to CHF (89%), either alone (82%) or associated with syncope (2%), ascites (14%) or bilateral hind limb paralysis as a result of ATE (2%). The remaining cats with clinical signs related to RCM had ascites (5%) or bilateral hind limb paralysis caused by ATE (6%).¹⁰¹ Cardiac auscultation was abnormal in 81% of 92 cats in that study, with 1-3 abnormalities for each. The most common abnormality was a left apical systolic heart murmur (77%), followed by gallop sound (31%) and arrhythmias (23%).¹⁰¹
RCM猫のほぼすべてが診断時に臨床徴候を示し、その大部分はCHFに関連する。¹⁷˒²¹˒²²˒¹⁰¹˒¹⁰⁴ 35例のRCM猫に関する報告では、91%がCHF、6%が嗜眠、3%が失神および一過性不全麻痺を呈した。¹⁷ 同様に、92例のRCM猫の研究では、70%が診断時に少なくとも1つのRCM関連臨床徴候を示した。¹⁰¹ 最も一般的な徴候はCHFに関連した呼吸困難(89%)であり、単独(82%)または失神(2%)、腹水(14%)、あるいはATEによる両側後肢麻痺(2%)を伴っていた。残りの臨床徴候を示した猫では、腹水(5%)またはATEによる両側後肢麻痺(6%)が認められた。¹⁰¹ 心臓聴診異常はこの研究の92例中81%で認められ、1〜3個の異常所見が存在した。最も一般的な異常は左心尖部収縮期雑音(77%)であり、続いて奔馬調律(31%)および不整脈(23%)であった。¹⁰¹
Electrocardiographic Findings:心電図所見
Various arrhythmias are associated with feline RCM, predominantly including ventricular premature beats or tachycardia (7-29%), supraventricular premature beats or tachycardia (4-23%), and third-degree AV block (5%).¹⁷˒¹⁰¹ Atrial fibrillation is reported less commonly (1-3%).¹⁷˒¹⁰¹
さまざまな不整脈が猫RCMと関連しており、主として心室性期外収縮または心室頻拍(7〜29%)、上室性期外収縮または上室頻拍(4〜23%)、およびIII度房室ブロック(5%)が含まれる。¹⁷˒¹⁰¹ 心房細動は比較的まれである(1〜3%)。¹⁷˒¹⁰¹
Clinical Course and Prognosis:臨床経過と予後
The prognosis for RCM in humans is poor, with most patients requiring cardiac transplantation.¹⁰⁷ Feline RCM is similarly associated with a poor prognosis, with most animals dying from cardiac-related causes (60-86%).¹⁷˒²¹˒²²˒¹⁰¹˒¹⁰⁴ For example, in one report, 64% of cats with RCM died from cardiac-related causes, with 16% occurring within the first 24 hours after the diagnosis was made.¹⁰¹ Most of these cats (92%) died or were euthanized because of refractory CHF (89%) or ATE (3%), while 8% died suddenly. Excluding cats that died <24 hours after diagnosis, the median survival time from diagnosis to all-cause death and cardiac death was 436 days (range, 2-3710 days) and 667 days (2-3710), respectively (Figure 234.9, F).¹⁰¹ Severe LAE (i.e., end-diastolic LA to aortic ratio [LA:Ao] ≥2; Video 234.13) was significantly associated with shorter time to cardiac death, independently of age, biatrial enlargement and arrhythmias.¹⁰¹ In another report, only respiratory distress showed a statistically significant effect on survival, with a median survival time of just 64 days (95% confidence interval = 8-120) for cats with respiratory distress vs. 466 days (95% confidence interval = 0-1208) for those without respiratory distress.¹⁰⁴
ヒトRCMの予後は不良であり、多くの患者で心臓移植が必要となる。¹⁰⁷ 猫RCMも同様に予後不良であり、多くの症例が心疾患関連死に至る(60〜86%)。¹⁷˒²¹˒²²˒¹⁰¹˒¹⁰⁴ 例えば、ある報告ではRCM猫の64%が心疾患関連死を呈し、そのうち16%は診断後24時間以内に死亡した。¹⁰¹ これらの猫の大部分(92%)は難治性CHF(89%)またはATE(3%)により死亡あるいは安楽死となり、8%は突然死であった。診断後24時間以内に死亡した猫を除外すると、診断から全死亡および心疾患関連死までの生存期間中央値は、それぞれ436日(範囲2〜3710日)および667日(2〜3710日)であった(図234.9, F)。¹⁰¹ 重度LAE(すなわち拡張末期LA/Ao比 ≥2;Video 234.13)は、年齢、両心房拡大、不整脈とは独立して、心疾患関連死までの期間短縮と有意に関連していた。¹⁰¹ 別の報告では、呼吸困難のみが生存に統計学的有意な影響を示し、呼吸困難を呈した猫の生存期間中央値はわずか64日(95%信頼区間=8〜120日)であったのに対し、呼吸困難を示さなかった猫では466日(95%信頼区間=0〜1208日)であった。¹⁰⁴
DILATED CARDIOMYOPATHY:拡張型心筋症
Definition—Prevalence:定義—有病率
DCM, a primary cardiomyopathy characterized by a dilated LV with systolic dysfunction (Figure 234.10),³˒⁸˒⁹⁴ was previously recognized as the second most common feline heart disease.¹ However, in 1987 Pion et al. demonstrated that most cases of feline DCM were actually not “primary,” but instead related to taurine deficiency (Video 234.14), and could be reversible and preventable with oral supplementation of taurine.¹⁰⁸˒¹⁰⁹ Since then, commercial cat foods have been supplemented with taurine. Other causes of DCM phenotypes such as sustained tachycardia are also reported.¹¹⁰ The prevalence of what was initially thought to be primary myocardial failure has thus decreased markedly, and DCM currently represents 5-10% of primary cardiomyopathies only.²⁰˒²² A large number of genetic causes of DCM has been recognized in humans, with most of the implicated genes encoding sarcomere, Z-disk, or cytoskeleton proteins.⁹⁴ Variants in the pyruvate kinase dehydrogenase 4 (PDK4) and titin (TTN) genes have also been identified in some Doberman Pinschers with DCM (ch. 233).¹¹¹ However, at the time of writing, no causal mutation has been identified for feline DCM, although genetic involvement with a complex pattern of inheritance was evidenced in a large colony of DSH cats.¹¹²
拡張型心筋症(DCM)は、左室拡張と収縮機能障害を特徴とする原発性心筋症であり(図234.10)、³˒⁸˒⁹⁴ 以前は猫で2番目に多い心疾患と認識されていた。¹ しかし1987年にPionらは、猫DCM症例の大部分が実際には“原発性”ではなくタウリン欠乏に関連しており(Video 234.14)、経口タウリン補充により可逆的かつ予防可能であることを示した。¹⁰⁸˒¹⁰⁹ それ以降、市販キャットフードにはタウリンが添加されるようになった。持続性頻脈など、DCM表現型を引き起こす他の原因も報告されている。¹¹⁰ 当初原発性心筋不全と考えられていた病態の有病率は著明に減少し、現在DCMは原発性心筋症の5〜10%を占めるに過ぎない。²⁰˒²² ヒトでは多数のDCM関連遺伝子が同定されており、その多くはサルコメア、Z帯、または細胞骨格蛋白をコードする。⁹⁴ Doberman Pinscherの一部では、pyruvate kinase dehydrogenase 4(PDK4)およびtitin(TTN)遺伝子変異も同定されている(第233章)。¹¹¹ しかし本稿執筆時点では、猫DCMに対する原因変異は同定されていない。ただし、DSH猫の大規模コロニーにおいて複雑な遺伝形式による遺伝的関与が示唆されている。¹¹²
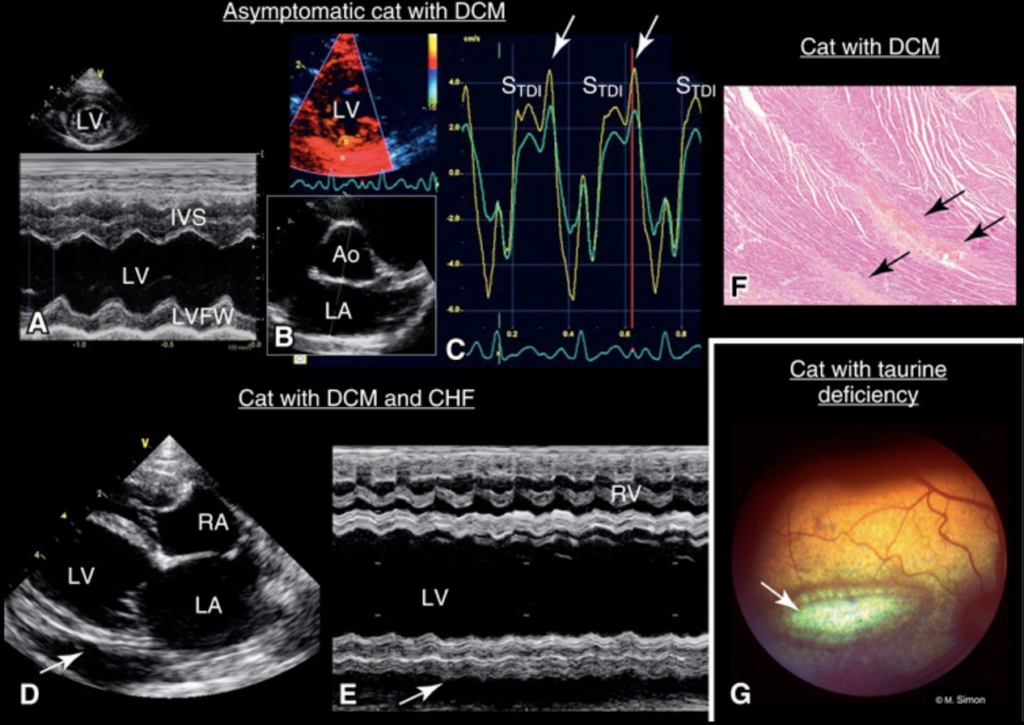
Findings in cats with dilated cardiomyopathy (DCM) and in a cat with taurine deficiency-induced myocardial failure.
拡張型心筋症(DCM)猫およびタウリン欠乏誘発性心筋不全猫における所見。
A-C, M-mode (A), two-dimensional (B), and color tissue Doppler (C) echocardiographic images from a Maine Coon cat with subclinical DCM.
A-C、不顕性DCMを有するメインクーン猫のMモード(A)、二次元(B)、およびカラー組織ドプラ(C)心エコー画像。
The cat was referred for echocardiographic examination before mating.
本症例は交配前の心エコー検査目的で紹介受診した。
(A) Myocardial failure is confirmed by a mildly decreased left ventricular fractional shortening (27%; reference interval, 33-66%).⁸⁸
(A)軽度低下した左室短縮率(27%;基準範囲 33–66%)⁸⁸により心筋不全が確認される。
B, The left atrial to aortic ratio is still normal (end-diastolic LA:Ao ratio = 1; reference interval, 0.5-1.2).⁸⁸
B、左房大動脈比はなお正常範囲内である(拡張末期LA:Ao比 = 1;基準範囲 0.5–1.2)。⁸⁸
(C) Radial myocardial velocity profiles of the left ventricular free wall (LVFW) show that the subendocardium (yellow) is moving more rapidly than the subepicardium (green) in both systole and diastole.
(C)左室自由壁(LVFW)の放射方向心筋速度プロファイルでは、収縮期および拡張期の両方において、心内膜下層(黄色)が心外膜下層(緑色)より速く動いていることが示される。
This defines systolic and diastolic radial myocardial velocity gradients; however, the mean systolic gradient (0.9 cm/s) is within the reference interval (2.2 ± 0.7 cm/s).⁸⁸
これは収縮期および拡張期の放射方向心筋速度勾配を示しているが、平均収縮期勾配(0.9 cm/s)は基準範囲内(2.2 ± 0.7 cm/s)である。⁸⁸
Post-systolic contraction waves (PSCs) (arrows), occur after S_TDI waves and are greater in amplitude than the latter; radial PSCs, defined as indicating abnormally delayed radial myocardial contractions occurring during early diastole (rather than during systole), were not observed in a population of 100 healthy cats.⁸⁸
収縮後収縮波(PSC)(矢印)はS_TDI波後に出現し、その振幅はS_TDI波より大きい。放射方向PSCは、収縮期ではなく拡張早期に生じる異常遅延性放射方向心筋収縮を示す所見として定義されるが、100頭の健常猫集団では認められなかった。⁸⁸
D-E, Echocardiographic images of a cat with DCM, and pleural effusion (arrows) due to congestive heart failure.
D-E、DCMおよびうっ血性心不全による胸水(矢印)を有する猫の心エコー画像。
The 4 cardiac chambers are dilated (D).
4心腔すべてが拡張している(D)。
Poor left ventricular function is confirmed by the low left ventricular fractional shortening (15%) and hypokinesis of the interventricular septum (IVS) and LVFW on the M-mode echocardiogram (E).
左室機能低下は、低い左室短縮率(15%)およびMモード心エコー図(E)上でのIVSおよびLVFWの運動低下により確認される。
F, Broad bands of replacement fibrosis (arrows, reddish-orange color) are seen, in addition to mild, diffuse interstitial fibrosis in a cat with DCM that died suddenly (hematoxylin-eosin-saffron stain, ×25).
F、突然死したDCM猫では、軽度びまん性間質性線維化に加えて、広範な置換性線維化帯(矢印、赤橙色)が認められる(ヘマトキシリン・エオジン・サフラン染色、×25)。
G, Right ocular fundus of a cat with central retinal degeneration due to taurine deficiency.
G、タウリン欠乏による中心性網膜変性を有する猫の右眼眼底。
Note the typical ellipsoid and hyperreflective lesion (arrow) with a pigmented border in the area centralis, i.e., lateral to the optic disc.
area centralis、すなわち視神経乳頭外側に、色素性辺縁を伴う典型的な楕円形高反射病変(矢印)が認められる。
Ao, aorta; LV, left ventricle; RA, right atrium; RV, right ventricle; S_TDI, peak myocardial velocity during systole.
Ao、大動脈;LV、左心室;RA、右心房;RV、右心室;S_TDI、収縮期最大心筋速度。
A-F, Courtesy Dr. Nathalie Cordonnier, Pathology Department, National Veterinary School of Alfort, France.
A-F、フランス・アルフォール国立獣医学校病理学教室 Nathalie Cordonnier博士提供。
G, Courtesy Dr. Marc Simon, Paris, France.
G、フランス・パリ Marc Simon博士提供。
Pathophysiological Consequences:病態生理学的帰結
As in humans and dogs,⁹⁴˒¹¹³ feline DCM is characterized by degenerative myocardial lesions of the LV or both ventricles, with various degrees of myocytolysis, fibrosis, coronary arteriosclerosis and some inflammatory infiltrates.¹ These lesions are responsible for decreased systolic function, with secondary systolic and then diastolic dilation of affected ventricles (Video 234.15). Dilation of the ventricular cavities commonly results in enlargement of the corresponding AV valve annulus, with secondary valve insufficiency potentially contributing to atrial dilation, subsequent CHF, and increased risk of ATE.²²˒¹¹⁴ In one report, valve insufficiency was apparent in 69% of 32 cats with DCM, with the MV and tricuspid valve (TV) affected concomitantly in half of the cases and spontaneous echo contrast in the LA of 9% of the cases.¹¹⁴
ヒトおよび犬と同様に、⁹⁴˒¹¹³ 猫DCMは左心室または両心室の変性性心筋病変を特徴とし、種々の程度の心筋融解、線維症、冠動脈硬化、および一部炎症性浸潤を伴う。¹ これらの病変により収縮機能低下が生じ、二次的に収縮期、続いて拡張期の心室拡張が進行する(Video 234.15)。心室腔拡張はしばしば対応する房室弁輪の拡大を引き起こし、二次的な弁閉鎖不全が心房拡張、その後のCHF、およびATEリスク増加に寄与する可能性がある。²²˒¹¹⁴ ある報告では、32例のDCM猫の69%で弁閉鎖不全が認められ、半数では僧帽弁(MV)と三尖弁(TV)が同時に障害され、9%では左心房内にspontaneous echo contrastが認められた。¹¹⁴
Epidemiology—Clinical Presentation at Diagnosis:疫学—診断時の臨床像
Females predominated in one report (8/11, 73%)²² but not another (11/32, 34%).¹¹⁴ Mean ages of 9.1 years (range, 2.0-15.5) and 10 years (range, 3-16) have been reported.²²˒¹¹⁴ Most DCM cats present with clinical signs of CHF at the time of diagnosis.²²˒¹¹⁴ These are predominantly dyspnea resulting from pleural effusion and/or pulmonary edema (69% and 34% of cases, respectively)¹¹⁴ and ascites (6/11 cases in one report).²² Signs of systemic hypotension (e.g., weakness) (55%),²² ATE (9%), and collapse (3%) also have been reported.¹²¹ Feline DCM also can be diagnosed incidentally in animals without clinical signs (Figure 234.10), indicating an occult (subclinical) phase of the disease, but currently this is not as well characterized as that of canine DCM.¹¹³ Cardiac auscultation abnormalities (ch. 38) are detected in the vast majority of cats with DCM (97%), including gallop sound (72%), systolic heart murmur (34%), muffled heart sounds (3%) and arrhythmias (28%).¹¹⁴
ある報告では雌が優勢であった(8/11、73%)²² が、別の報告ではそうではなかった(11/32、34%)。¹¹⁴ 平均年齢として9.1歳(範囲2.0〜15.5歳)および10歳(範囲3〜16歳)が報告されている。²²˒¹¹⁴ DCM猫の大部分は診断時にCHF徴候を呈する。²²˒¹¹⁴ 主徴候は胸水および/または肺水腫に起因する呼吸困難であり(それぞれ69%および34%)、¹¹⁴ 腹水(ある報告では11例中6例)も認められる。²² 全身性低血圧徴候(例:虚弱)(55%)、²² ATE(9%)、虚脱(3%)も報告されている。¹²¹ 猫DCMは臨床徴候を示さない動物で偶発的に診断されることもあり(図234.10)、潜在性(subclinical)病期の存在を示しているが、現在のところ犬DCMほど詳細には特徴づけられていない。¹¹³ 心臓聴診異常(第38章)はDCM猫の大多数(97%)で認められ、奔馬調律(72%)、収縮期心雑音(34%)、心音減弱(3%)、不整脈(28%)が含まれる。¹¹⁴
Electrocardiographic Findings:心電図所見
Most ECG tracings from cats with DCM are abnormal.²⁰˒²² Nonspecific morphological ECG alterations resulting from cardiac chamber enlargement are commonly found.²⁰˒²² Various arrhythmias (ch. 230) are also frequently diagnosed, predominantly including ventricular premature complexes and supraventricular tachycardia.¹¹⁴ As with HCM and RCM, AF is much less common (1/11 in one case series).²⁰
DCM猫のECG波形の大部分は異常を示す。²⁰˒²² 心腔拡大に起因する非特異的形態学的ECG変化が一般的に認められる。²⁰˒²² さまざまな不整脈(第230章)も頻繁に診断され、主として心室性期外収縮および上室頻拍が含まれる。¹¹⁴ HCMおよびRCMと同様に、AFははるかにまれである(ある症例群では11例中1例)。²⁰
Clinical Course and Prognosis:臨床経過と予後
Among cats with primary cardiomyopathies, those with DCM have one of the shortest survival times.²²˒¹¹⁵ A median survival time of 11 days has been reported.²² In a retrospective comparative study, the median survival time of cats with DCM was 49 days (range, 1 to >502) if they received inotropic therapy (pimobendan) plus standard therapy (furosemide, taurine, ACE inhibitor, and/or digoxin), vs. 12 days (range, 1-244) for cats receiving the standard therapy alone.¹¹⁴ In most cases, death was due to euthanasia for refractory CHF (42%) or ATE (19%), and a high proportion of sudden death was also reported (36%; Figure 234.10, F).¹¹⁴ Hypothermia at presentation (<37.2°C) and LV FS% <20% were both associated with reduced survival.¹¹⁴
原発性心筋症の猫の中で、DCM猫は最も短い生存期間を示す群の1つである。²²˒¹¹⁵ 生存期間中央値11日との報告がある。²² 後ろ向き比較研究では、強心療法(ピモベンダン)に標準療法(フロセミド、タウリン、ACE阻害薬、および/またはジゴキシン)を追加した猫では生存期間中央値49日(範囲1〜>502日)であったのに対し、標準療法単独群では12日(範囲1〜244日)であった。¹¹⁴ 多くの症例で死亡原因は難治性CHFによる安楽死(42%)またはATE(19%)であり、高率の突然死(36%;図234.10, F)も報告されている。¹¹⁴ 初診時低体温(<37.2°C)および左室FS% <20%は、いずれも生存期間短縮と関連していた。¹¹⁴
Arrhythmogenic Right Ventricular Cardiomyopathy:不整脈原性右室心筋症
Definitions—Comparative Knowledge in Humans and Small Animals:定義―ヒトおよび小動物における比較知識
Human:ヒト
Human ARVC is predominantly a rare, genetically-determined cardiomyopathy. It affects the RV primarily, and pathologically it is characterized by fibrofatty replacement of RV myocytes, leading to RV dysfunction and failure, ventricular tachyarrhythmias, and increased risk of sudden cardiac death.¹¹⁶⁻¹²⁰ In early stages of the disease, structural myocardial changes are mild and confined to localized RV areas.¹¹⁷˒¹¹⁸ At a later stage, RV myocardial fibrofatty lesions become diffuse, with potential involvement of the LV.¹¹⁸ Besides this “classic right-dominant form” of the disease, two less common forms are reported: a biventricular form and a left-dominant form characterized by early occurrence of LV involvement, while RV remains preserved.¹¹⁸ Owing to these biventricular and left-dominant subtypes, the term ARVC does not strictly reflect actual myocardial lesions, explaining why the broader term “arrhythmogenic ventricular cardiomyopathy” has been proposed.¹¹⁸ Nowadays, ARVC is known as an acquired heart disease with a causal mutation in genes encoding proteins of the intercalated disc, mainly desmosomal proteins (e.g., plakoglobin, desmoplakin, desmocollin-2, plakophilin-2, and desmoglein-2) in >60% of patients.¹¹⁶⁻¹¹⁸ The cardiac desmosome plays various important roles, as it supports structural stability of the myocardium, maintains proper electrical stability and conductivity through regulation of gap junctions and calcium homeostasis, and regulates transcription of genes involved in adipogenesis and apoptosis.¹¹⁷ The genetically-determined disruption of desmosomal integrity in ARVC therefore results in myocyte detachment, apoptosis, and necrosis, with inflammatory infiltration (as a reactive process to cardiac death), and subsequent fibrofatty replacement (presumed to represent a “reparative” myocardial process).¹¹⁷˒¹¹⁸ These lesions result in atrophy of the RV myocardial wall, with secondary RV hypokinesis and dilation, potentially leading to TV regurgitation and RA enlargement, and right-sided CHF can occur. Disruption of desmosomal integrity also promotes ventricular arrhythmias at early stages of the disease, owing to electrical instability and alteration in myocyte electrical coupling.¹¹⁸˒¹¹⁹ Myocardial inflammation associated with ARVC could also represent immune or infectious mechanisms. A predisposition of human patients with ARVC to viral or bacterial myocarditis has been suggested, and myocarditis is known to potentially mimic ARVC lesions. However, the link between myocarditis and ARVC remains to be clarified.¹²⁰
ヒトのARVCは、主として稀な遺伝性心筋症である。主に右心室(RV)を侵し、病理学的にはRV心筋細胞の線維脂肪性置換を特徴とし、その結果としてRV機能障害および右心不全、心室性頻脈性不整脈、ならびに突然心臓死リスクの増加をもたらす。¹¹⁶⁻¹²⁰ 疾患早期では、構造的心筋変化は軽度であり、限局性のRV領域に限られる。¹¹⁷˒¹¹⁸ 疾患進行期には、RV心筋の線維脂肪性病変はびまん性となり、左心室(LV)への進展も認められる。¹¹⁸ この「古典的右室優位型」に加えて、より稀な2つの病型、すなわち両心室型および左室優位型が報告されている。左室優位型では、RVが比較的保たれる一方で、LV病変が早期から出現する。¹¹⁸ これら両心室型および左室優位型の存在により、「ARVC」という用語は実際の心筋病変を厳密には反映していないことから、より包括的な「不整脈原性心室心筋症(arrhythmogenic ventricular cardiomyopathy)」という名称が提唱されている。¹¹⁸現在では、ARVCは介在板蛋白をコードする遺伝子変異に起因する疾患として認識されており、患者の60%以上でデスモソーム蛋白(プラコグロビン、デスモプラキン、デスモコリン-2、プラコフィリン-2、デスモグレイン-2など)の異常が認められる。¹¹⁶⁻¹¹⁸ 心筋デスモソームは、心筋構造の安定性維持、ギャップ結合およびカルシウム恒常性調節を介した電気的安定性・伝導性維持、さらには脂肪形成やアポトーシス関連遺伝子転写調節など、多様な重要機能を担っている。¹¹⁷ そのため、ARVCにおける遺伝的なデスモソーム機能破綻は、心筋細胞の剥離、アポトーシスおよび壊死を引き起こし、これに反応性炎症細胞浸潤が加わり、その後の線維脂肪性置換(修復過程を反映すると考えられる)へと進行する。¹¹⁷˒¹¹⁸これら病変はRV心筋壁の萎縮をもたらし、二次的にRV低運動および拡張を生じ、三尖弁逆流(TV regurgitation)や右房(RA)拡大を引き起こし、右側うっ血性心不全(CHF)へ進展しうる。また、デスモソーム機能破綻は、電気的不安定性および心筋細胞間電気結合異常を介して、疾患早期から心室性不整脈を促進する。¹¹⁸˒¹¹⁹ARVCに伴う心筋炎症は、免疫学的あるいは感染性機序を反映している可能性もある。ARVC患者ではウイルス性あるいは細菌性心筋炎への素因が示唆されており、また心筋炎病変はARVC病変を模倣しうることが知られている。しかし、心筋炎とARVCとの関連は未だ明確ではない。¹²⁰
Small Animals:小動物
Spontaneous AVRC is reported in the dog,¹²¹⁻¹²⁸ and is a familial disease in the Boxer breed (autosomal dominant trait, incomplete and age-related penetrance) frequently associated with the deletion in the striatin gene on chromosome 17 (ch. 233).¹²⁴˒¹²⁵ Striatin is located at the intercalated disc region of cardiomyocytes and co-localized with other desmosomal proteins involved in the pathogenesis of human ARVC.¹¹⁶⁻¹¹⁸ In the cat, ARVC is a recently recognized cardiomyopathy, accounting for <5% of all myocardial diseases (Figure 234.11).¹˒²⁰˒¹²⁹ A series of 12 cases of feline ARVC was described extensively in 2000.¹⁵ Since then, a few sporadic cases have been reported.¹³⁰⁻¹³² At the time of writing, unlike human and canine ARVC, no genetic transmission has been identified in association with feline ARVC; therefore, its origin remains unproven. In the series of 12 cats with ARVC,¹⁵ morphological lesions were similar to those described in humans, including diffuse (7/12) or segmental (5/12) thinning of the RV wall, RV aneurysms of varying degrees (6/12 cats), and RA enlargement (7/12 cats) (Video 234.16). Histological lesions were also similar to those of human ARVC, including marked RV myocardial atrophy with fibrous or fibrofatty (9/12) and fatty (3/12) replacement in all cats, and apoptosis and focal or multifocal myocarditis in 9/12 and 10/12 cats, respectively. As described in humans and dogs,¹¹⁸˒¹²¹ similar lesions were observed in the LV of most cats (10/12), and even severe LV involvement has been reported.¹³¹
自然発生性ARVCは犬で報告されており、¹²¹⁻¹²⁸ ボクサー犬では家族性疾患として認識されている(常染色体優性遺伝、不完全かつ年齢依存性浸透率)。本疾患はしばしば第17染色体上のstriatin遺伝子欠失と関連する(第233章)。¹²⁴˒¹²⁵ Striatinは心筋細胞の介在板領域に存在し、ヒトARVC病態形成に関与する他のデスモソーム蛋白と共局在する。¹¹⁶⁻¹¹⁸猫では、ARVCは近年認識された心筋症であり、全心筋疾患の5%未満を占める(図234.11)。¹˒²⁰˒¹²⁹ 猫ARVCの12症例シリーズが2000年に詳細に報告された。¹⁵ 以降、散発症例が少数報告されている。¹³⁰⁻¹³² 本稿執筆時点では、ヒトや犬のARVCとは異なり、猫ARVCにおける遺伝的伝播は確認されておらず、その起源は未解明である。12例の猫ARVCシリーズでは、¹⁵ 形態学的病変はヒトARVCに類似しており、びまん性(7/12)または区域性(5/12)のRV壁菲薄化、程度様々なRV瘤形成(6/12)、およびRA拡大(7/12)が認められた(Video 234.16)。組織学的病変もヒトARVCと類似しており、全例で著明なRV心筋萎縮と線維性あるいは線維脂肪性置換(9/12)、または脂肪性置換(3/12)が認められた。さらに、アポトーシスおよび限局性または多発性心筋炎が、それぞれ9/12例および10/12例で認められた。ヒトおよび犬と同様に、¹¹⁸˒¹²¹ 多くの猫(10/12)でLVにも類似病変が認められ、重度LV病変例も報告されている。¹³¹
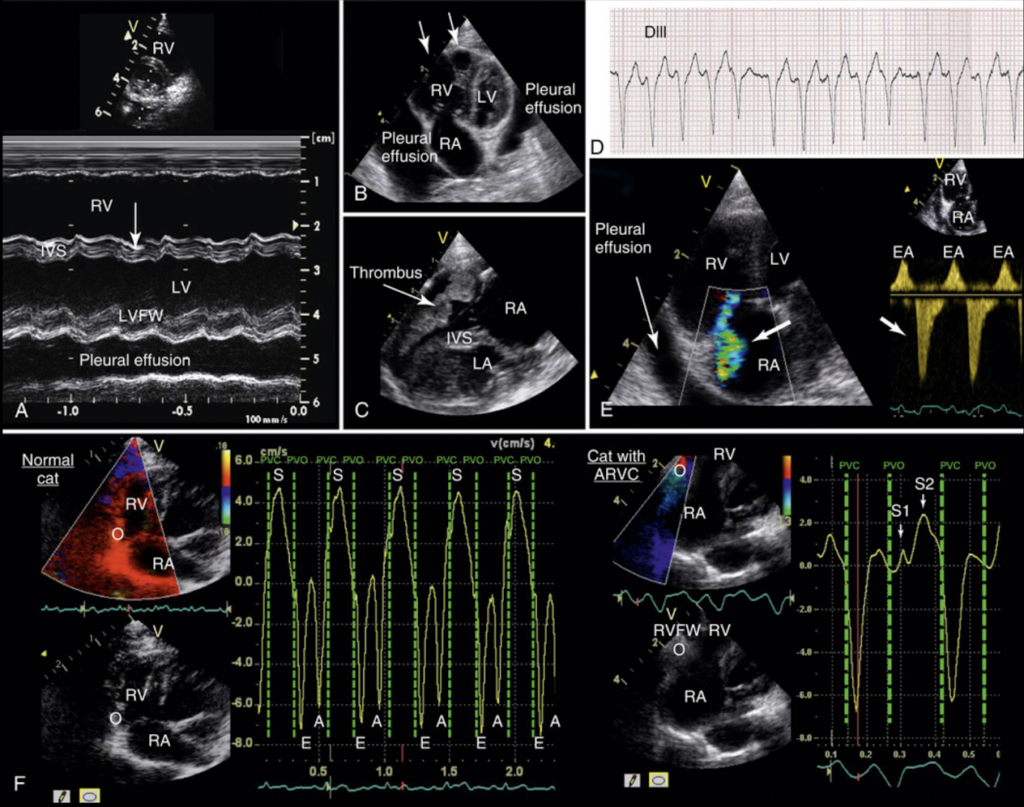
Representative findings in 4 cats with arrhythmogenic right ventricular cardiomyopathy (ARVC).
不整脈原性右室心筋症(ARVC)を有する4頭の猫における代表的所見。
A, M-mode echocardiographic image confirming severe right ventricular dilation with paradoxical motion (arrow) of the interventricular septum (IVS) in a cat with ARVC.
A、ARVC猫において、心室中隔(IVS)の奇異性運動(矢印)を伴う重度右室拡張を確認したMモード心エコー画像。
Pleural effusion is a sign of congestive heart failure.
胸水はうっ血性心不全の徴候である。
LV, Left ventricle; LVFW, left ventricular free wall; RV, right ventricle.
LV、左心室;LVFW、左室自由壁;RV、右心室。
B, Two-dimensional echocardiographic image showing severe aneurismal right ventricular dilation (arrows), marked right atrial enlargement, and pleural effusion, in another cat with ARVC.
B、別のARVC猫において、重度の瘤状右室拡張(矢印)、著明な右房拡大、および胸水を示す二次元心エコー画像。
LV, Left ventricle; RA, right atrium; RV, right ventricle.
LV、左心室;RA、右心房;RV、右心室。
C, Two-dimensional echocardiographic image obtained from a third cat with ARVC (right parasternal 4-chamber view) showing severe right atrial and right ventricular dilation, with a voluminous thrombus in the right ventricular cavity.
C、3頭目のARVC猫から得られた二次元心エコー画像(右傍胸骨四腔断面像)であり、重度の右房および右室拡張と、右室腔内の大きな血栓を示している。
IVS, Interventricular septum; LA, left atrium; RA, right atrium.
IVS、心室中隔;LA、左心房;RA、右心房。
D, Atrial fibrillation with right bundle branch block morphology in a cat with severe ARVC (same animal as in panel A). 25 mm/s, 2 cm = 1 mV.
D、重度ARVC猫(Aパネルと同一症例)における、右脚ブロック型波形を伴う心房細動。25 mm/s、2 cm = 1 mV。
E, Tricuspid insufficiency (thick arrows) documented with color-flow (left panel) and continuous-wave (right panel) Doppler echocardiography in a fourth cat with ARVC.
E、4頭目のARVC猫において、カラーフロードプラ(左パネル)および連続波ドプラ(右パネル)心エコー検査で確認された三尖弁閉鎖不全(太矢印)。
There is marked enlargement of the right cardiac chambers.
右心系心腔の著明な拡大が認められる。
EA, Fused early (E) and late (A) diastolic tricuspid waves; LV, left ventricle; RA, right atrium; RV, right ventricle.
EA、融合した早期(E)および後期(A)拡張期三尖弁波;LV、左心室;RA、右心房;RV、右心室。
F, Color tissue Doppler echocardiographic imaging of a cat with arrhythmogenic right ventricular cardiomyopathy (ARVC) (right, same cat as in panel B; left, a normal cat for comparison).
F、不整脈原性右室心筋症(ARVC)猫のカラー組織ドプラ心エコー画像(右:Bパネルと同一症例、左:比較用正常猫)。
In the diseased cat, evidence of severe right ventricular myocardial systolic dysfunction includes an abnormal double systolic wave (S1 and S2), with a decreased and delayed peak systolic wave (S2) occurring at end-systole, instead of mid-systole (S).
罹患猫では、重度右室心筋収縮機能障害の所見として、異常な二峰性収縮期波(S1およびS2)が認められ、収縮中期(S)ではなく収縮終期に、低下かつ遅延した収縮期最大波(S2)が出現している。
RA, Right atrium; RV, right ventricle; RVFW, right ventricular free wall; S, E, and A, peak velocities of the right myocardial wall during systole, early diastole, and late diastole, respectively.
RA、右心房;RV、右心室;RVFW、右室自由壁;S、E、およびAは、それぞれ収縮期、拡張早期、および拡張後期における右心筋壁の最大速度を示す。
Epidemiology—Clinical Presentation at Diagnosis:疫学―診断時の臨床像
Most cats with ARVC are middle-aged at diagnosis (mean age = 7.3 years),¹⁵ even though the age range is wide (1-20 years).¹⁵˒¹³⁰˒¹³¹ No breed or sex predisposition has been reported. The familial aspect of the disease has been evoked, but not demonstrated.¹²⁹ Most cats with ARVC show signs of right-sided CHF at presentation (Figure 234.11).¹⁵˒¹³⁰˒¹³¹ Syncope related to ventricular tachyarrhythmias is a less common clinical expression.¹⁵˒¹²⁹ As in humans and dogs, cats with ARVC may have subclinical disease for a variable period of time. The disease can thus be diagnosed in apparently healthy cats referred for echocardiography, mainly because of an abnormal cardiac auscultation (heart murmur and/or arrhythmias).¹²⁹˒¹³² A soft, right-sided apical systolic heart murmur consistent with TV regurgitation is detected in most cases (8/12 cats in one series).¹⁵˒¹²⁹ Arrhythmias may also be detected. Heart sounds may be muffled in cases of pericardial or pleural effusion.¹²⁹˒¹³⁰ Nonspecific general signs (e.g., lethargy, anorexia) are also reported, even in those without evidence of CHF.¹⁵˒¹²⁹
ARVC猫の多くは中年齢で診断される(平均年齢7.3歳)が、¹⁵ 年齢幅は広い(1〜20歳)。¹⁵˒¹³⁰˒¹³¹ 品種素因や性差は報告されていない。家族性疾患である可能性は示唆されているものの、証明はされていない。¹²⁹多くのARVC猫は、初診時に右側CHF徴候を呈する(図234.11)。¹⁵˒¹³⁰˒¹³¹ 心室性頻脈性不整脈に関連した失神は比較的稀な臨床徴候である。¹⁵˒¹²⁹ ヒトおよび犬と同様に、猫ARVCでも一定期間無症候性に経過する場合がある。そのため、主として心雑音や不整脈などの異常心音聴取を契機に心エコー検査へ紹介された、一見健康な猫で診断されることもある。¹²⁹˒¹³²多くの症例では、三尖弁逆流に一致する右側心尖部収縮期雑音が聴取される(あるシリーズでは8/12例)。¹⁵˒¹²⁹ 不整脈も認められることがある。心膜液貯留や胸水が存在する場合には、心音減弱を認める。¹²⁹˒¹³⁰ また、CHFの証拠がない場合でも、元気消失や食欲不振などの非特異的全身症状が報告されている。¹⁵˒¹²⁹
Electrocardiographic Findings:心電図所見
As reported in humans and dogs, cats with ARVC display a large variety of ECG alterations, including ventricular premature complexes/tachycardia of RV and LV origin (particularly with LV involvement), AF, supraventricular tachycardia, right bundle branch block, and first- and third-degree AV blocks (Figure 234.11, D).¹⁵˒¹²⁹˒¹³⁰
ヒトおよび犬で報告されているように、猫ARVCでも多様なECG異常が認められる。これには、RVおよびLV起源の心室性期外収縮・心室頻拍(特にLV病変を伴う場合)、心房細動(AF)、上室性頻拍、右脚ブロック、ならびにⅠ度およびⅢ度房室ブロックが含まれる(図234.11,D)。¹⁵˒¹²⁹˒¹³⁰
Clinical Course and Prognosis:臨床経過と予後
Although cats with ARVC may have subclinical disease for an unknown duration, the prognosis of overt ARVC is usually poor. Most cats with ARVC-related CHF die days or weeks after the diagnosis is made, due to cardiac reasons (spontaneous death or euthanasia due to worsening or unresponsive CHF and/or ATE despite therapy).¹⁵˒¹²⁹˒¹³⁰ In a series of 12 cats with ARVC, 6 died of CHF 2 days to 4 months after onset of clinical signs (median = 1 month).¹⁵
ARVC猫では一定期間無症候性に経過することがあるものの、顕性ARVCの予後は一般的に不良である。ARVC関連CHFを呈した猫の多くは、診断後数日から数週間以内に、心原性死亡(突然死、あるいは治療抵抗性CHFやATE悪化による安楽死)に至る。¹⁵˒¹²⁹˒¹³⁰
12例のARVCシリーズでは、6例が臨床徴候出現後2日〜4か月以内にCHFで死亡しており、中央値は1か月であった。¹⁵
NONSPECIFIC CARDIOMYOPATHIES:非特異的心筋症
This category (previously named “unclassified cardiomyopathies”) is reserved for cardiomyopathies that do not fit under other headings (HCM, RCM, DCM, and ARVC).³ In other words, NSCM does not characterize a single distinct myocardial disease, but instead encompasses the uncommon primary cardiomyopathies whose echocardiographic characteristics do not correspond to the typical features of the 4 well-defined cardiomyopathies described above. In cats, echocardiographic examination most commonly reveals a mix of alterations including segmental LVH, regional hypokinesis, and marked LAE.⁴ In humans, primary NSCM also includes other forms of cardiomyopathies, e.g., myocardial noncompaction, which has been reported in the cat.¹¹˒³¹˒³²˒¹³³ Although of unclear pathogenesis, at least some NSCM could represent particular forms or stages of other cardiomyopathies (e.g., HCM), as a result of more or less extensive areas of myocardial ischemia and/or infarction (secondary to coronary arteriosclerosis, decreased coronary blood flow secondary to increased LV filling pressure, functional coronary constriction, inadequate capillary density related to increased myocardial mass, and/or coronary vascular thromboembolism).¹³⁴⁻¹³⁷ The follow-up of human and feline HCM patients has thus highlighted a “dilated” HCM stage characterized by LV dilation, relative thinning of LV myocardial walls, diffuse or regional decreased contractility, and usually severe LAE (Table 234.1).¹³⁵⁻¹³⁸ In addition to the role of myocardial ischemia and/or infarction, apoptosis and genetic mutations have been evoked to explain this phenotypic HCM evolution in humans.¹³⁹˒¹⁴⁰ These particular HCM forms are also characterized by multifocal myocardial scarring with large regions of replacement fibrosis that can mimic RCM lesions.¹³⁷ Therefore, the diagnosis of NSCM should be established with caution and the hypothesis of evolution of another primary cardiomyopathy, in particular HCM or RCM, should first be ruled out. However, a differential diagnosis may be difficult to establish in the absence of previous sequential echocardiographic examinations. In one feline study, NSCM represented only 10% of 106 primary cardiomyopathies.²² Most affected cats were adult females, with a mean age of 8.8 ± 4.8 (0.8-15 years) and more than half presented with signs of CHF. Surprisingly, a greater survival time was observed for cats with NSCM (925 days) as compared with HCM (492 days), RCM (132 days) and DCM (11 days).
このカテゴリー(以前は「分類不能型心筋症」と呼称)は、他の分類(HCM、RCM、DCM、ARVC)に該当しない心筋症に対して用いられる。³ すなわち、NSCMは単一の独立した心筋疾患を意味するものではなく、上記4つの明確な心筋症に典型的には一致しない心エコー所見を示す稀な原発性心筋症群を包含する概念である。猫では、心エコー検査において区域性LVH、局所壁運動低下、著明な左房拡大(LAE)などの混合性変化を認めることが多い。⁴ ヒトでは、原発性NSCMには心筋緻密化障害(myocardial noncompaction)なども含まれ、猫でも報告されている。¹¹˒³¹˒³²˒¹³³病因は明確ではないものの、少なくとも一部のNSCMは、HCMなど他の心筋症の特殊型あるいは進行段階を反映している可能性がある。これは、冠動脈硬化、LV充満圧上昇に伴う冠血流低下、機能的冠攣縮、心筋肥大に伴う毛細血管密度低下、あるいは冠血管血栓塞栓症などに起因する、心筋虚血および/または梗塞領域の広がりによると考えられている。¹³⁴⁻¹³⁷ヒトおよび猫のHCM症例追跡研究では、LV拡張、LV壁相対的菲薄化、びまん性または局所性収縮能低下、通常は重度LAEを特徴とする「拡張型HCM」段階が明らかとなっている(Table 234.1)。¹³⁵⁻¹³⁸ このようなHCM表現型進展には、心筋虚血・梗塞に加え、アポトーシスや遺伝子変異も関与すると考えられている。¹³⁹˒¹⁴⁰ これら特殊型HCMでは、多発性心筋瘢痕および広範な置換性線維化を認め、RCM病変を模倣しうる。¹³⁷したがって、NSCM診断は慎重に行う必要があり、とくにHCMやRCMなど他の原発性心筋症の進行形態である可能性をまず除外すべきである。しかし、過去の連続的心エコー検査データが存在しない場合、鑑別診断は困難となることがある。ある猫の研究では、NSCMは106例の原発性心筋症中10%のみを占めた。²² 多くは成猫雌であり、平均年齢は8.8 ± 4.8歳(0.8〜15歳)で、半数以上がCHF徴候を呈していた。興味深いことに、NSCM猫の生存期間(925日)は、HCM(492日)、RCM(132日)、DCM(11日)よりも長かった。
SECONDARY CARDIOMYOPATHIES:二次性心筋症
The final diagnosis of any primary cardiomyopathy should be established after exclusion of secondary cardiomyopathies characterized by similar phenotypes (Table 234.1).³ Therefore, the ACVIM Consensus Statement recommends to screen for possible underlying causes of cardiomyopathy phenotypes when such phenotypes have been diagnosed echocardiographically.³ For instance, hyperthyroidism (ch. 287) is common in older cats, potentially leading to LV remodeling or exacerbating LVH of cats with preexisting HCM (ch. 287).³˒¹⁴¹⁻¹⁴⁴ Therefore, according to the ACVIM Consensus Statement,³ serum thyroxine concentrations should be measured in all cats ≥6 years of age with LVH, as well as in those with cardiac auscultation abnormalities such as a murmur (ch. 38), gallop (Audio 38.5), or arrhythmias (ch. 230), whether they have LVH or not. Hyperthyroidism should also be ruled out in cats that have an RCM phenotype.³ Similarly, systemic arterial blood pressure (ch. 91) should be measured in all cats with an HCM phenotype,³ as diffuse (or less commonly segmental) LVH is observed in up to 85% of hypertensive cats (ch. 236).¹⁴⁵⁻¹⁴⁸ Systemic hypertension, which is common in elderly cats, may also worsen LVH in the case of preexisting HCM.³
原発性心筋症の最終診断は、類似表現型を示す二次性心筋症を除外した後に確定すべきである(Table 234.1)。³ そのため、ACVIMコンセンサスステートメントでは、心エコー検査により心筋症表現型が認められた場合、基礎疾患検索を推奨している。³例えば、甲状腺機能亢進症(第287章)は高齢猫で一般的であり、LVリモデリングや、既存HCM猫におけるLVH悪化を引き起こしうる(第287章)。³˒¹⁴¹⁻¹⁴⁴ したがって、ACVIMコンセンサスステートメントでは、LVHを有する6歳以上の猫すべて、およびLVHの有無にかかわらず心雑音(第38章)、奔馬調律(Audio 38.5)、不整脈(第230章)などの心音異常を有する猫において、血清サイロキシン濃度測定を推奨している。³ RCM表現型を示す猫でも、甲状腺機能亢進症除外が必要である。³同様に、HCM表現型を有するすべての猫では全身血圧測定(第91章)が推奨される。³ 高血圧猫では、最大85%にびまん性(あるいはまれに区域性)LVHが認められるためである(第236章)。¹⁴⁵⁻¹⁴⁸ 高齢猫に一般的な全身性高血圧は、既存HCM症例におけるLVH悪化要因ともなりうる。³
Other potential pathological causes of LVH that should be considered include congenital aortic stenosis (ch. 231), hypovolemia (pseudohypertrophy),¹⁴⁹ infiltrative tumor (e.g., lymphoma; ch. 322),³˒¹⁵⁰ myocarditis of various causes (e.g., Bartonella spp. [ch. 191], FIV [ch. 198], and Toxoplasma [ch. 197]),¹⁵¹⁻¹⁵³ muscular dystrophy,¹⁵⁴˒¹⁵⁵ steroid-associated CHF,¹⁵⁶ acromegaly (ch. 280),¹⁵⁷⁻¹⁶⁰ and transient LV wall thickening.¹⁶¹ LVH is common in diabetic cats with hypersomatotropism (72%), and this so called “acromegalic cardiomyopathy” is reversible in most cases after hypophysectomy and normalization of circulating insulin-like growth factor 1 (IGF-1) concentrations.¹⁶⁰ Interestingly, elevated IGF-1 concentrations have also been found in a small proportion of non-diabetic cats with HCM (7%), raising the question of its impact on LV remodeling.¹⁵⁹ Transient myocardial thickening has been described in cats with CHF.¹⁶¹ This spontaneously resolving form of myocardial change can mimic HCM. It preferentially affects younger cats (median age, 2 years; range, 0.4-11) and often (71%) follows an antecedent event (e.g., general anesthesia, road accident, vaccination, bite wound, pneumonia, fever of unknown origin, with different drugs and drug combinations administered concomitantly).¹⁶¹ The long-term prognosis of transient myocardial thickening is much better than that of decompensated HCM, as cardiac treatment can be discontinued in most affected cats (95%), with decrease and even normalization of both LV myocardial wall thicknesses and LA:Ao ratio within a mean of 3 months.¹⁶¹ The underlying cause of such transient LVH is still unknown, but myocardial edema and transient cellular infiltration related to acute myocarditis is suspected.¹⁶¹
LVHの他の潜在的原因としては、先天性大動脈狭窄(第231章)、循環血液量減少(偽性肥大)、¹⁴⁹ 浸潤性腫瘍(リンパ腫など;第322章)、³˒¹⁵⁰ 各種心筋炎(Bartonella spp.[第191章]、FIV[第198章]、Toxoplasma[第197章]など)、¹⁵¹⁻¹⁵³ 筋ジストロフィー、¹⁵⁴˒¹⁵⁵ ステロイド関連CHF、¹⁵⁶ 先端巨大症(第280章)、¹⁵⁷⁻¹⁶⁰ 一過性LV壁肥厚などが挙げられる。¹⁶¹糖尿病性高ソマトトロピン症猫ではLVHが一般的(72%)であり、この「先端巨大症性心筋症」は、下垂体摘出術およびIGF-1濃度正常化後、多くで可逆的である。¹⁶⁰ 興味深いことに、非糖尿病性HCM猫の一部(7%)でもIGF-1高値が認められており、そのLVリモデリングへの関与が示唆されている。¹⁵⁹一過性心筋肥厚はCHF猫でも報告されている。¹⁶¹ この自然軽快性心筋変化はHCMを模倣しうる。若齢猫(中央値2歳、範囲0.4〜11歳)に多く、しばしば(71%)先行イベント(全身麻酔、交通事故、ワクチン接種、咬傷、肺炎、不明熱、多剤併用など)に続発する。¹⁶¹一過性心筋肥厚の長期予後は非代償性HCMよりはるかに良好であり、多くの症例(95%)で心臓治療中止が可能となる。平均3か月以内にLV壁厚およびLA:Ao比の低下、さらには正常化が認められる。¹⁶¹ この一過性LVHの原因は依然不明であるが、急性心筋炎に関連した心筋浮腫および一過性細胞浸潤が疑われている。¹⁶¹
Lastly, in cases of the DCM phenotype, the differential diagnosis should include taurine deficiency,¹⁰⁸˒¹⁰⁹ drug toxicosis (e.g., doxorubicin), or sustained tachyarrhythmia.³˒¹¹⁰
最後に、DCM表現型症例では、タウリン欠乏、¹⁰⁸˒¹⁰⁹ 薬物中毒(ドキソルビシンなど)、あるいは持続性頻脈性不整脈を鑑別診断に含めるべきである。³˒¹¹⁰
DIAGNOSTIC APPROACH TO FELINE PRIMARY CARDIOMYOPATHIES:猫の原発性心筋症に対する診断アプローチ
PHYSICAL EXAMINATION:身体検査
Cardiomyopathy should be suspected in cats with abnormal cardiac auscultation (systolic heart murmur, gallop sound, arrhythmias; chs. 38, 230), and in those with clinical signs of CHF (ch. 229), ATE (ch. 238), syncope (ch. 40), and/or weakness (ch. 23). However, the absence of auscultatory abnormality does not preclude cardiomyopathy, as cardiac auscultation may be normal in some affected cats, with heart murmurs less commonly found in cats with CHF.¹⁶² Furthermore, many cats with heart murmur do not suffer from cardiomyopathy. In a prospective study of 780 apparently healthy cats (the CatScan study), the prevalence of heart murmurs was high (41%), but most heart murmurs (70%) were considered functional, i.e., associated with a normal echocardiogram.⁴⁷ The positive predictive value of a heart murmur for indicating HCM was only 18% for cats aged <1 year, 25 to 30% between 1 year and 9 years, and 43% in senior cats (≥9 years).⁴⁷ Nevertheless, the presence of a grade 3/6 or 4/6 heart murmur is suggestive of HCM, whereas grade 5 or 6/6 heart murmurs (i.e., associated with a palpable thrill) are more often related to congenital cardiac disorders.³˒⁴⁷ Gallop sounds (ch. 38) and arrhythmias (ch. 230) are also highly suggestive of myocardial disease, and compared to heart murmurs, gallop sounds and arrhythmias are noted more often in cats with CHF.³˒¹⁶²
心筋症は、心臓聴診異常(収縮期心雑音、ギャロップ音、不整脈;第38章、第230章)を有する猫、ならびにCHF(第229章)、ATE(第238章)、失神(第40章)、および/または虚弱(第23章)の臨床徴候を示す猫で疑うべきである。しかし、聴診異常が存在しないからといって心筋症を除外することはできない。罹患猫の一部では心臓聴診が正常である場合があり、CHFを有する猫では心雑音が認められる頻度は比較的低い。¹⁶² さらに、心雑音を有する多くの猫は心筋症を有していない。780頭の一見健康な猫を対象とした前向き研究(CatScan study)では、心雑音の有病率は高率(41%)であったが、その大部分(70%)は機能性雑音、すなわち正常心エコー検査と関連するものと判断された。⁴⁷ HCMを示唆する心雑音の陽性的中率は、1歳未満では18%、1〜9歳では25〜30%、高齢猫(9歳以上)では43%に過ぎなかった。⁴⁷ それでもなお、グレード3/6または4/6の心雑音はHCMを示唆する。一方、グレード5または6/6の心雑音(すなわち触知可能なスリルを伴うもの)は、先天性心疾患と関連することがより多い。³˒⁴⁷ ギャロップ音(第38章)および不整脈(第230章)もまた心筋疾患を強く示唆する所見であり、心雑音と比較すると、CHFを有する猫ではギャロップ音や不整脈の方がより高頻度に認められる。³˒¹⁶²
Clinical signs of CHF include dyspnea/tachypnea (related to pulmonary edema, pleural effusion, or both; ch. 37), with frequent paradoxical breathing in the case of pleural effusion (ch. 229).¹⁶³ Ascites is less common as a manifestation of CHF in cats. Pleural effusion (ch. 220) may be associated with muffled heart or lung sounds, and pulmonary edema with respiratory crackles. The RAPID CAT study, dedicated to cats with acute dyspnea, demonstrated that gallop sounds, hypothermia (rectal temperature <37.5°C [<99.5°F]), tachycardia (heart rate >200 bpm) and respiratory rate >80 breaths per minute were all useful to predict cardiac-associated dyspnea.¹⁶⁴
CHFの臨床徴候には呼吸困難/頻呼吸が含まれ、これは肺水腫、胸水、またはその両方に関連する(第37章)。胸水症例では逆説性呼吸を高頻度に伴う(第229章)。¹⁶³ 猫におけるCHFの症状として腹水は比較的少ない。胸水(第220章)は心音または肺音減弱を伴うことがあり、肺水腫では捻髪音が聴取される場合がある。急性呼吸困難猫を対象としたRAPID CAT studyでは、ギャロップ音、低体温(直腸温 <37.5°C[<99.5°F])、頻脈(心拍数 >200 bpm)、および呼吸数 >80回/分が、心原性呼吸困難を予測するうえで有用であることが示された。¹⁶⁴
THORACIC RADIOGRAPHY:胸部X線検査
Cardiomegaly:心拡大
Cardiomegaly is the most common radiographic abnormality associated with feline cardiomyopathies (Figure 234.12).¹⁶⁵⁻¹⁶⁷ As in dogs, the vertebral heart score (VHS) may be used for objectively assessing and comparing heart size in sequential radiographs. The reference interval is 7.5 ± 0.3 vertebrae (v) on a lateral projection; typically accepted upper limits are ≤8.1 and 9 v on lateral and dorsoventral or ventrodorsal views, respectively, with very few breed variations (unlike dogs).¹⁶⁷⁻¹⁶⁹ However, thoracic radiographs present some diagnostic limitations. Cats with subclinical HCM that consists of mild to moderate LVH and no LAE do not show any radiographic changes. Additionally, and similarly to dogs, pulmonary edema or pleural effusion can obscure the margins of the cardiac silhouette, precluding accurate evaluation of heart size and shape. Thus, VHS is relatively specific but not sensitive to predict cardiac enlargement in cats.¹⁶⁷ For example, with a VHS cutoff >8.2 v on lateral views, the specificity for predicting any degree of LAE is reported as 92%, but the sensitivity ranges from 63-78% in cats with mild to severe LAE, respectively.¹⁶⁷ With the same cutoff, the specificity for distinguishing cats with left-sided heart diseases from healthy cats was reported as 100%, but the sensitivity was only 52%.¹⁶⁷ Nevertheless, VHS remains a useful tool to help differentiate cardiac from non-cardiac causes of respiratory distress in emergency situations when echocardiography is not immediately available or technically achievable. In cases of acute dyspnea, a VHS >9.3 v on lateral radiographs is highly specific for presence of an underlying heart disease.¹⁷⁰
心拡大は、猫の心筋症に関連する最も一般的なX線異常所見である(図234.12)。¹⁶⁵⁻¹⁶⁷ 犬と同様に、vertebral heart score(VHS)を用いて、連続撮影されたX線写真上で心サイズを客観的に評価・比較することが可能である。基準範囲は側面像で7.5 ± 0.3椎体(v)であり、一般に受け入れられている上限値は、側面像で≤8.1 v、背腹像または腹背像で9 vである。犬と異なり、品種差はほとんど認められない。¹⁶⁷⁻¹⁶⁹ しかし、胸部X線検査にはいくつかの診断上の限界が存在する。軽度〜中等度のLVHを有し、LAEを伴わない潜在性HCMでは、X線学的変化が認められない。また、犬と同様に、肺水腫や胸水によって心陰影辺縁が不明瞭となり、心サイズや形状の正確な評価が困難となる。そのため、VHSは猫の心拡大予測に対して比較的特異度は高いが、感度は低い。¹⁶⁷ 例えば、側面像におけるVHSカットオフ値を>8.2 vとした場合、LAEの予測に対する特異度は92%と報告されているが、感度は軽度〜重度LAE症例でそれぞれ63〜78%であった。¹⁶⁷ 同じカットオフ値を用いた場合、左心系疾患猫と健康猫を鑑別する特異度は100%であったが、感度は52%に過ぎなかった。¹⁶⁷ それでもなお、VHSは、心エコー検査が直ちに利用できない、あるいは技術的に実施困難な救急状況において、呼吸困難の心原性/非心原性鑑別を補助する有用な指標である。急性呼吸困難猫では、側面像でVHS >9.3 vは、基礎心疾患の存在に対して非常に高い特異度を有する。¹⁷⁰
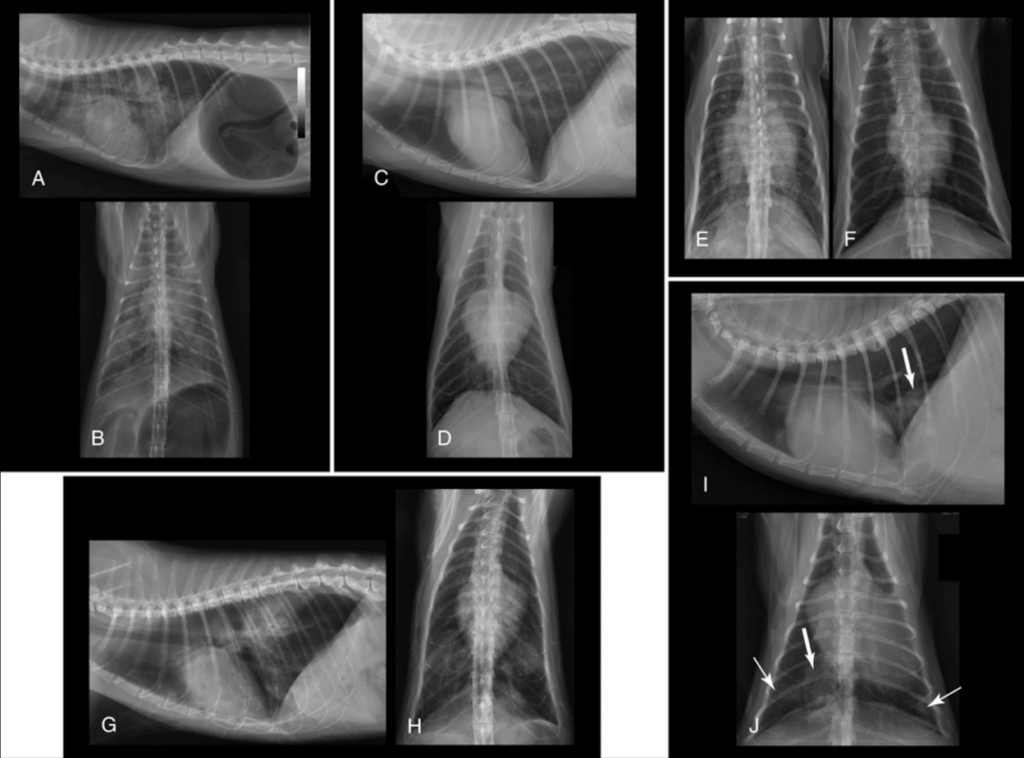
Thoracic radiographs obtained from cats with various cardiomyopathies.
さまざまな心筋症を有する猫から得られた胸部X線画像。
A-B (hypertrophic cardiomyopathy [HCM]): right lateral (R lat) and dorsoventral (DV) projections showing marked cardiomegaly (vertebral heart score [VHS], 8.9) on R lat and a valentine-shaped heart (DV).
A-B(肥大型心筋症[HCM]):右側面像(R lat)および背腹像(DV)であり、右側面像では著明な心拡大(vertebral heart score[VHS]、8.9)、DV像ではバレンタイン型心陰影を示している。
An echocardiogram confirmed severe left atrial (LA) enlargement without right atrial (RA) enlargement.
心エコー検査では、右房(RA)拡大を伴わない重度左房(LA)拡大が確認された。
The alveolar lung pattern with a symmetrical, mainly cranioventral and caudoventral distribution, is consistent with cardiogenic pulmonary edema.
対称性で主として前腹側および後腹側に分布する肺胞性肺パターンは、心原性肺水腫と一致する。
Severe gas distension of the stomach due to aerophagia, and diaphragmatic flattening, are consistent with respiratory distress.
空気嚥下による重度胃内ガス貯留および横隔膜平坦化は、呼吸困難と一致する所見である。
C-D (HCM): these projections show severe cardiomegaly (VHS = 9.4 on R lat) and a valentine-shaped heart on the ventrodorsal (VD) projection.
C-D(HCM):これらの投影像では、重度心拡大(R latでVHS = 9.4)および腹背像(VD)でのバレンタイン型心陰影が認められる。
An echocardiogram confirmed severe LA enlargement (end-diastolic LA:Ao = 2.2; reference interval, 0.5-1.2)⁸⁸ without RA enlargement.
心エコー検査では、RA拡大を伴わない重度LA拡大(拡張末期LA:Ao = 2.2;基準範囲 0.5–1.2)⁸⁸が確認された。
Here, pulmonary edema is characterized by a diffuse uniform unstructured interstitial lung pattern.
ここでは、肺水腫はびまん性で均一な非構造性間質性肺パターンとして特徴づけられる。
E (HCM): in this DV projection, marked enlargement of the pulmonary vessels is seen, in comparison to the thickness of the ninth rib where they cross each other.
E(HCM):このDV像では、第9肋骨との交差部における肋骨厚と比較して、肺血管の著明な拡張が認められる。
There is a marked increase in width of the cardiac silhouette (> two-thirds that of the thorax), without a valentine-shaped heart.
バレンタイン型心陰影を伴わずに、心陰影幅の著明な増加(胸郭幅の3分の2超)が認められる。
Cardiogenic pulmonary edema is characterized by a marked diffuse unstructured interstitial lung pattern.
心原性肺水腫は、著明なびまん性非構造性間質性肺パターンを特徴とする。
F (same cat as in panel E): the VD projection obtained 1 day later after treatment with furosemide shows regression of pulmonary infiltrates, a decreased size of the cardiac silhouette, but persistent enlargement of the pulmonary vessels.
F(Eパネルと同一症例):フロセミド治療1日後に撮影されたVD像では、肺浸潤影の改善、心陰影サイズの縮小が認められるが、肺血管拡張は持続している。
G-H (restrictive cardiomyopathy): there is severe cardiomegaly (VHS, 9.2 on R lat) and a valentine-shaped heart (VD).
G-H(拘束型心筋症):重度心拡大(R latでVHS 9.2)およびバレンタイン型心陰影(VD)が認められる。
An echocardiogram demonstrated severe enlargement of only the LA (end-diastolic LA:Ao = 1.7).
心エコー検査では、左房のみの重度拡大(拡張末期LA:Ao = 1.7)が確認された。
There is a multifocal, patchy alveolar infiltrate in the cranioventral and caudodorsal lung fields consistent with pulmonary edema.
前腹側および後背側肺野に、多発性かつ斑状の肺胞性浸潤影が認められ、肺水腫と一致する。
There is no perihilar distribution as seen in the dog.
犬でみられるような肺門周囲分布は認められない。
I-J (arrhythmogenic right ventricular cardiomyopathy): there is increased sternal contact (R lat) and a left cardiac shift (VD) consistent with right-sided cardiomegaly.
I-J(不整脈原性右室心筋症):胸骨接触の増加(R lat)および左側への心偏位(VD)が認められ、右心系心拡大と一致する。
The VHS is increased (9.0).
VHSは増加している(9.0)。
Marked enlargement of the caudal vena cava (thick arrows) is also seen (twice the height of the thoracic aorta).
後大静脈の著明な拡張(太矢印)も認められ(胸部大動脈径の2倍)、
There are 2 alveolar patches in the caudal lung lobes (thin arrows); differentials to consider include pulmonary edema or pulmonary thromboembolism.
後肺葉には2か所の肺胞性陰影(細矢印)が認められ、鑑別診断として肺水腫または肺血栓塞栓症が考慮される。
Courtesy Dr. Pascaline Pey, Diagnostic Imaging Department, National Veterinary School of Alfort, France.
フランス・アルフォール国立獣医学校画像診断学教室 Pascaline Pey博士提供。
Cardiac Shape:心臓形態
The typical valentine-shaped heart, assessed on dorsoventral or ventrodorsal views (Figure 234.12,D) was initially considered to be related to biatrial enlargement and relatively specific to feline HCM.¹˒¹⁶⁶˒¹⁷¹˒¹⁷² However, a strong positive correlation between LA size and severity of the valentine shape was demonstrated, without any effect of RA size on the latter, except when concurrent with severe LAE.¹⁷² Similarly, in another report, the majority (83%) of cats with valentine-shaped heart had a cardiomyopathy, but only 32% had HCM (RCM and NSCM accounting for 17% and 34% of the remaining cases, Figure 234.12,H), with biatrial enlargement confirmed in only one-third of cats.¹⁷¹ In both reports, 10-19% of cats with a valentine-shaped heart were diagnosed with conditions other than cardiomyopathies (e.g., congenital heart diseases and volume overload), and up to 7% did not even show any echocardiographic abnormality.¹⁷¹˒¹⁷² Therefore, the valentine-shaped heart should no longer be considered as a specific feature of feline HCM, nor does it predict the presence of biatrial enlargement, as its primary cause is LAE.¹⁷¹˒¹⁷² For ARVC specifically, thoracic radiographs typically show enlargement of the cardiac silhouette related to RV and RA dilation, frequently associated with a dilated caudal vena cava (Figures 234.12, I and J).¹˒¹⁵˒¹²⁹ Global heart enlargement can also be seen in cases of pericardial effusion and/or concurrent dilation of the left heart chambers.
背腹像または腹背像で評価される典型的なバレンタイン型心陰影(図234.12,D)は、当初、両心房拡大と関連し、猫HCMに比較的特異的であると考えられていた。¹˒¹⁶⁶˒¹⁷¹˒¹⁷² しかし、左房サイズとバレンタイン形状の重症度との間には強い正の相関が認められた一方で、重度LAEを伴う場合を除き、右房サイズはこの形状に影響しないことが示された。¹⁷² 同様に、別の報告では、バレンタイン型心陰影を呈した猫の大多数(83%)は心筋症を有していたが、そのうちHCMは32%のみであり、残りはRCMおよびNSCMがそれぞれ17%および34%を占めていた(図234.12,H)。また、両心房拡大が確認されたのは全体の3分の1に過ぎなかった。¹⁷¹ 両報告において、バレンタイン型心陰影を呈した猫の10〜19%は心筋症以外の疾患(先天性心疾患や容量負荷など)と診断され、さらに最大7%では心エコー異常すら認められなかった。¹⁷¹˒¹⁷² したがって、バレンタイン型心陰影はもはや猫HCMに特異的な所見とは考えるべきではなく、その主因がLAEであることから、両心房拡大の存在を予測するものでもない。¹⁷¹˒¹⁷²ARVCでは、胸部X線検査において、RVおよびRA拡張に関連した心陰影拡大が典型的に認められ、しばしば後大静脈拡張を伴う(図234.12,IおよびJ)。¹˒¹⁵˒¹²⁹ また、心膜液貯留や左心系拡張を併発する症例では、全体的な心拡大が認められる場合もある。
Signs of CHF:CHF徴候
As in dogs, radiography is considered the gold standard for confirming thoracic signs of CHF, including vascular enlargement, pulmonary edema, and/or pleural effusion. Thoracic radiographs usually show pleural effusion in cats with decompensated ARVC, whereas pulmonary edema is more commonly diagnosed than pleural effusion in cats with decompensated HCM (66% vs. 34%, Figure 234.12, A-E).⁴⁴ Unlike dogs, the perihilar to caudodorsal distribution of cardiogenic pulmonary edema does not predominate in cats. Pulmonary edema related to CHF is instead characterized by an increased lung opacity with a range of mixed patterns of variable distribution. In one study of 23 cats with CHF, diffuse (uniform or non-uniform) distribution was the most common, and all cats had evidence of a reticular or granular interstitial pattern.¹⁷³ Diffuse interstitial patterns may be similar to those associated with chronic bronchitis (Figures 234.12, C and D), which can be confusing (ch. 215). A ventral distribution is also common (Figure 234.12, A), mimicking pulmonary opacities related to bronchopneumonia (ch. 217), and leading to another risk of misdiagnosis.¹⁷³
犬と同様に、X線検査は血管拡張、肺水腫、および/または胸水を含むCHFの胸郭内徴候を確認するためのゴールドスタンダードと考えられている。胸部X線検査では、非代償性ARVC猫では通常胸水が認められる。一方、非代償性HCM猫では胸水よりも肺水腫の方が高頻度に診断される(66% vs. 34%、図234.12,A-E)。⁴⁴ 犬とは異なり、猫では心原性肺水腫が肺門部から尾背側に優位に分布することは少ない。CHF関連肺水腫は、むしろ分布が多様な混合性パターンを伴う肺透過性低下として特徴づけられる。CHFを有する23頭の猫を対象とした研究では、び漫性分布(均一または不均一)が最も一般的であり、全症例で網状または顆粒状の間質性パターンが認められた。¹⁷³ び漫性間質性パターンは慢性気管支炎に伴う所見(図234.12,CおよびD)と類似する場合があり、鑑別を困難にする可能性がある(第215章)。また、腹側分布も一般的であり(図234.12,A)、気管支肺炎(第217章)に伴う肺陰影と類似し、誤診のリスクとなる。¹⁷³
For cats with acute dyspnea, for which thoracic radiographs cannot be obtained safely, other diagnostic modalities should be used instead until the cat is stabilized.³˒¹⁷⁴˒¹⁷⁵ A combination of point-of-care diagnostic techniques (lung ultrasound assessing the presence of B-lines, focused cardiac ultrasound evaluating LA size and presence of pleural effusion, and NT-proBNP test) is recommended.³˒¹⁷⁴˒¹⁷⁵
急性呼吸困難猫では、安全に胸部X線撮影を行えない場合があり、その際は状態安定化まで他の診断モダリティを優先すべきである。³˒¹⁷⁴˒¹⁷⁵ B-lineの有無を評価する肺超音波、LAサイズおよび胸水の有無を評価するフォーカス心エコー、ならびにNT-proBNP測定を組み合わせたPOCUSベースの診断アプローチが推奨されている。³˒¹⁷⁴˒¹⁷⁵
ECHOCARDIOGRAPHIC EXAMINATION(TABLES 234.3 AND 234.4; CH. 97):心エコー検査(表234.3および234.4;第97章)
TABLE 234.3 Main Indications for Echocardiography in Cats³
表234.3 猫における心エコー検査の主な適応³
| HISTORY – EPIDEMIOLOGY 病歴・疫学 | PHYSICAL EXAMINATION 身体検査 | OTHERS その他 |
|---|---|---|
|
1. Clinical signs reported by the owner and commonly associated with CM (e.g., dyspnea, exercise intolerance, syncope, weakness) 1. オーナーから報告され、CMと一般的に関連する臨床徴候(例:呼吸困難、運動不耐性、失神、虚弱) 2. Seizures (without any other neurological abnormalities) 2. 発作(その他の神経学的異常を伴わない) 3. Family history of CM or sudden death 3. CMまたは突然死の家族歴 4. Maine Coon or Ragdoll cats with a MyBPC3 mutation but also without* 4. MyBPC3変異を有するメインクーンまたはラグドール、または変異を有しない場合も含む* 5. Any endocrine disease (specifically hyperthyroidism, diabetes mellitus) 5. 何らかの内分泌疾患(特に甲状腺機能亢進症、糖尿病) 6. Fever of unknown origin 6. 原因不明熱 7. Intolerance to parenteral fluid administration or general anesthesia 7. 非経口輸液投与または全身麻酔に対する不耐性 |
1. Abnormal cardiac auscultation (systolic heart murmur, gallop sound, arrhythmia, muffled heart sounds) 1. 心臓聴診異常(収縮期心雑音、ギャロップ音、不整脈、心音減弱) 2. Clinical signs suggestive of CHF (e.g., dyspnea/tachypnea, paradoxical breathing, ascites) 2. CHFを示唆する臨床徴候(例:呼吸困難/頻呼吸、奇異性呼吸、腹水) 3. Clinical signs of arterial thromboembolism (e.g., acute paralysis/paresis, absent femoral arterial pulse, etc.) 3. 動脈血栓塞栓症の臨床徴候(例:急性麻痺/不全麻痺、大腿動脈拍動の消失など) |
1. Cats ≥9 years old for which a procedure known to potentially precipitate CHF is planned (e.g., general anesthesia, parenteral fluid administration, extended-release glucocorticoids) 1. CHFを誘発する可能性が知られている処置が予定されている9歳以上の猫(例:全身麻酔、非経口輸液投与、持続放出型グルココルチコイド) 2. Pedigree breeding cat 2. 血統繁殖猫 |
CHF、うっ血性心不全;CM、心筋症。
Some Maine Coon and Ragdoll cats negative for MyBPC3 mutations (A31P and R820W, respectively) have been reported with hypertrophic cardiomyopathy. Therefore, cats from these breeds should undergo regular echocardiographic screening.³,⁴²,⁵⁴
MyBPC3変異(それぞれA31PおよびR820W)陰性である一部のメインクーンおよびラグドールでも、肥大型心筋症が報告されている。したがって、これらの品種の猫では定期的な心エコー検査スクリーニングを受けるべきである。³,⁴²,⁵⁴
Modified from the American College of Veterinary Internal Medicine Consensus Statement on Feline Cardiomyopathies.³
American College of Veterinary Internal Medicine(ACVIM)による猫心筋症コンセンサスステートメントより改変。³
Indications and Recommended Protocols:適応および推奨プロトコール
Echocardiography combined with Doppler examination (Videos 234.3 to 234.16) is the most accurate non-invasive tool to identify myocardial diseases and assess myocardial phenotypes (HCM, RCM, DCM, and NSCM). Main indications are presented in Table 234.3. The ACVIM Consensus Statement recommends three echocardiographic protocols (from basic to advanced) according to practical circumstances.³ The “focused-point-of-care” protocol, consisting of noting the presence of pleural or pericardial effusion and pulmonary B-lines, and subjectively evaluating LA size and motion as well as LV systolic function, is recommended for unstable patients (ch. 73).³ The “focused-point-of-care” protocol can also be used by operators with minimal training when the two other protocols are not possible, as it provides information on the presence of moderate to marked changes associated with cardiomyopathy and the risk for CHF or ATE.³˒¹⁷⁶ The “standard of care” protocol performed by trained operators includes M-mode and 2D measurements (see below) with qualitative assessment of LV papillary muscle size, and presence or absence of SAM, mid-LV obstruction, regional wall motion abnormalities, and spontaneous echo contrast or thrombus.³ The “best practice protocol” refers to echocardiographic examination conducted by cardiologists who are experts in echocardiography and includes spectral Doppler and TDI measurements in addition to the “standard of care” protocol.³
ドプラ検査を組み合わせた心エコー検査(Videos 234.3〜234.16)は、心筋疾患を同定し、心筋フェノタイプ(HCM、RCM、DCM、NSCM)を評価するための、最も正確な非侵襲的検査法である。主な適応はTable 234.3に示されている。ACVIMコンセンサスステートメントでは、実際の状況に応じて、基本的なものから高度なものまで3種類の心エコープロトコールを推奨している。³“focused-point-of-care”プロトコールは、胸水または心嚢液の有無、肺B-lineの有無を確認し、さらに左心房(LA)の大きさおよび動態、左室(LV)収縮機能を主観的に評価するものであり、不安定な症例に推奨される(第73章)。³この“focused-point-of-care”プロトコールは、他の2つのプロトコールが実施不可能な場合には、最小限のトレーニングしか受けていない術者でも使用可能である。これは、心筋症に関連する中等度から重度の変化や、CHFまたはATEのリスクに関する情報を提供するためである。³˒¹⁷⁶訓練を受けた術者によって実施される“standard of care”プロトコールには、Mモードおよび2D計測(後述)が含まれ、さらにLV乳頭筋サイズ、SAMの有無、中部LV閉塞、局所壁運動異常、自発性エコーコントラストまたは血栓の有無について定性的評価を行う。³“best practice protocol”は、心エコー検査の専門家である循環器専門医によって実施される心エコー検査を指し、“standard of care”プロトコールに加えて、スペクトラルドプラおよびTDI測定を含む。³
Two-Dimensional and M-Mode Measurements:二次元法およびMモード計測
The following basic principles and recommendations should be considered in order to limit the risk of misdiagnosis:
誤診リスクを低減するために、以下の基本原則および推奨事項を考慮すべきである。
Pulsed-Wave Doppler Mode:パルス波ドプラモード
Pulsed-wave Doppler mode provides surrogate measures of LV diastolic function (e.g., mitral inflow velocities, deceleration time of early transmitral flow [E], isovolumic relaxation time). In cats with HCM and RCM, these are often used together with mitral annular velocities assessed by pulsed-wave TDI (Figure 234.9), because early mitral annular velocity (Ea) and the E:Ea ratio are considered surrogate measures of LV relaxation and filling pressure (Table 234.4).⁷⁴
パルス波ドプラモードは、LV拡張機能の代替指標(僧帽弁流入速度、初期僧帽弁流入波[E波]の減速時間、等容性弛緩時間など)を提供する。HCMおよびRCMの猫では、これらの指標は、パルス波TDIによって評価された僧帽弁輪速度(Figure 234.9)と併用されることが多い。これは、早期僧帽弁輪速度(Ea)およびE:Ea比が、LV弛緩能および充満圧の代替指標と考えられているためである(Table 234.4)。⁷⁴
Pulsed-wave Doppler mode can also be used for assessing LA appendage flow velocity, cats with low flow velocities being at risk for spontaneous echo contrast and possible subsequent ATE.³˒⁷⁶
パルス波ドプラモードは、LA耳介血流速度の評価にも利用可能であり、低流速を示す猫では、自発性エコーコントラストおよびその後のATE発症リスクが高い。³˒⁷⁶
Lastly, continuous-wave and color-flow Doppler modes are used to assess dynamic LVOTO and AV valve regurgitations (Table 234.4 and Figure 234.8) (ch. 97).
最後に、連続波ドプラおよびカラーフロードプラモードは、動的LVOTOおよび房室弁逆流の評価に用いられる(Table 234.4およびFigure 234.8)(第97章)。
TABLE 234.4 Echocardiographic Diagnostic Characteristics of the 4 Main Feline Cardiomyopathies (see also Figures 234.3, 234.6, and 234.8-234.11)*
表234.4 4つの主要な猫心筋症の心エコー診断学的特徴(図234.3、234.6、および234.8–234.11も参照)*
| 英語 | 日本語 | Cardiomyopathy Phenotypes / 心筋症表現型 | |||
|---|---|---|---|---|---|
| Hypertrophic Cardiomyopathy | Restrictive Cardiomyopathy | Dilated Cardiomyopathy | ARVC | ||
| 2D and M-mode | 2DおよびMモード |
Most common features and specific forms • Diffuse or segmental, symmetric or asymmetric concentric LV hypertrophy and/or IVS ≥6 mm at end-diastole • Hypertrophy of papillary muscles • Possible LV cavity obliteration at end-systole • Normal to ↑ systolic LV function • LAE with ↓ LA FS at later stages • OHCM: hypertrophy of subaortic IVS and SAM of MV leaflets and/or chordae tendineae resulting in DLVOTO |
• Severe LAE or LAE + RAE; ↓ LA FS at later stages • LVFW, IVS thicknesses within reference range • LV FS% within reference range • Focal or diffuse hyperechoic myocardial and endocardial areas (fibrosis) • EMF specific form with bridging scar between LVFW and IVS and/or diffuse circumferential hyperechoic endocardial thickening with reduced LV cavity (rare) |
• Increased diastolic and systolic LV internal diameters • Decreased LV FS% (<30%) • Thinning of LVFW, IVS, and/or papillary muscles • Increased MV EPSS (>4 mm) • LAE with ↓ LA FS at later stages |
• Severe RA, RV enlargement • Paradoxical IVS motion • Diffuse or segmental thinning of RVMW with hypokinesis, akinesis and/or dyskinesis • Abnormal RVW trabeculation (esp. apical) • Focal to large RV aneurysm (esp. at apex and subtricuspid region) |
|
最も一般的な所見および特異的病型 • びまん性または区域性、対称性または非対称性の求心性左室肥大、および/または拡張末期IVS ≥6 mm • 乳頭筋肥大 • 収縮終期における左室腔閉塞の可能性 • 正常〜増加した左室収縮機能 • 進行期では左房拡大および左房短縮率低下 • 閉塞性HCM:大動脈弁下IVS肥厚および僧帽弁尖/腱索のSAMにより動的左室流出路閉塞を生じる |
• 重度左房拡大、または左房+右房拡大;進行期では左房短縮率低下 • 左室自由壁およびIVS厚は基準範囲内 • 左室短縮率は基準範囲内 • 局所性またはびまん性の高エコー性心筋・心内膜領域(線維化) • EMF特異型ではLVFWとIVSを連結する瘢痕、および/または左室腔縮小を伴うびまん性円周状高エコー性心内膜肥厚 |
• 左室拡張期および収縮期内径増大 • 左室短縮率低下(<30%) • 左室自由壁、IVS、および/または乳頭筋菲薄化 • 僧帽弁EPSS増加(>4 mm) • 進行期で左房拡大および左房短縮率低下 |
• 重度右房・右室拡大 • 奇異性IVS運動 • 右室自由壁のびまん性または区域性菲薄化と低運動、無運動、および/または奇異運動 • 異常な右室肉柱形成(特に心尖部) • 局所性〜大型右室瘤(特に心尖部および三尖弁下領域) | ||
| Pulsed-wave Doppler mode | パルス波ドプラモード |
Mitral inflow Relaxation pattern: inverted E:A ratio (<1), ↑ EDT and IVRT (>60 ms) | Restrictive pattern: ↑ E:A ratio (>2) with ↑ E wave and ↓ A wave, shortened EDT and IVRT (<34 ms) | Variable patterns depending on LVFP and loading conditions. Restrictive pattern possible at end-stages with ↑ LA pressure | |
| Mitral inflow | 僧帽弁流入血流 | 弛緩障害パターン:E:A比逆転(<1)、EDTおよびIVRT延長(>60 ms) | 拘束型パターン:E波増加、A波低下を伴うE:A比増加(>2)、EDTおよびIVRT短縮(<34 ms) | 左室充満圧および前負荷条件に依存した多様なパターン。終末期では左房圧上昇に伴い拘束型パターンを示す可能性 | |
| Pulmonary vein inflow | 肺静脈流入 | Systolic-dominant flow pattern with prominent AR wave (and Adur:ARdur ratio >1 if LVFP still normal) | SD reversal (diastolic-dominant flow pattern) with a small or absent AR wave (and Adur:ARdur ratio <1) predictive of poor LA contraction | ||
| 肺静脈流入 | 肺静脈流入 | 収縮期優位血流パターンと顕著なAR波(左室充満圧正常時にはAdur:ARdur比 >1) | SD逆転(拡張期優位血流パターン)および小さい、または消失したAR波(Adur:ARdur比 <1)は左房収縮不全を示唆 | ||
| Mitral annulus pulsed-wave TDI | 僧帽弁輪パルス波TDI | Low diastolic waves (Ea <6 cm/s) but normal mitral E:Ea ratio (<12) if LVFP not yet elevated | Low diastolic waves, Ea <6 cm/s, with inverted (<1) or normal (>1) Ea:Aa ratio associated with E:Ea ratio >12 | ||
| 僧帽弁輪パルス波TDI | 僧帽弁輪パルス波TDI | 拡張期波低下(Ea <6 cm/s)だが、左室充満圧未上昇時にはE:Ea比正常(<12) | 拡張期波低下(Ea <6 cm/s)、E:Ea比 >12 を伴うEa:Aa比逆転(<1)または正常(>1) | ||
| Color-flow Doppler mode | カラーフロードプラ |
• MR • OHCM: 2 turbulent systolic jets (LVOT and posteriorly-directed aliased jet of MR) |
• MR • EMF with bridging scar: systolic obstruction of mid-LV cavity | Mild to moderate MR and/or TR owing to atrioventricular annular dilation | Mild to moderate TR |
| カラーフロードプラ | カラーフロードプラ |
• 僧帽弁逆流 • 閉塞性HCM:2本の乱流性収縮期ジェット(LVOTおよび後方偏位したMRジェット) |
• 僧帽弁逆流 • ブリッジ瘢痕を伴うEMF:左室中央部収縮期閉塞 | 房室弁輪拡張に伴う軽度〜中等度MRおよび/またはTR | 軽度〜中等度TR |
The fifth one, nonspecific cardiomyopathy, includes cases whose echocardiographic features do not fit readily into the 4 defined types.
5番目の非特異的心筋症には、心エコー所見が4つの定義済み病型に明確には当てはまらない症例が含まれる。
Other ultrasound imaging features include signs of congestive heart failure (e.g., B-lines, pleural and pericardial effusion, dilatation of the caudal vena cava and ascites), and spontaneous echo contrast or thrombus in dilated atrial chambers.
その他の超音波画像所見として、うっ血性心不全徴候(例:Bライン、胸水・心嚢液、後大静脈拡張、腹水)や、拡張した心房内の自然エコーコントラストまたは血栓が含まれる。2D, Two-dimensional; A, peak velocity of late diastolic transmitral flow; Aa, peak velocity of late diastolic mitral annular motion as assessed by pulsed-wave TDI; Adur, duration of mitral A wave; AR, peak velocity of pulmonary vein flow reversal during atrial contraction; ARdur, duration of the AR wave; Aₜᴅɪ, peak myocardial velocity assessed by 2D color TDI during late diastole; D, peak velocity of diastolic pulmonary vein flow; DLVOTO, dynamic left ventricular outflow tract obstruction; E, peak velocity of early diastolic transmitral flow; Ea, peak velocity of early diastolic mitral annular motion as assessed by pulsed-wave TDI; E DT, mitral E wave deceleration time; EMF, endomyocardial form of restrictive cardiomyopathy; EPSS, E-point-to-septal separation; ES, end-systole; Eₜᴅɪ, peak myocardial velocity assessed by 2D color TDI during early diastole; esp, especially; FS%, fractional shortening; IVRT, isovolumic relaxation time; IVS, interventricular septum; LA, left atrium/atrial; LAE, left atrial enlargement; LV, left ventricle/ventricular; LVFP, left ventricular filling pressure; LVFW, left ventricular free wall; LVH, left ventricular hypertrophy; LVOT, left ventricular outflow tract; MR, mitral regurgitation; MV, mitral valve; MVG, myocardial velocity gradients assessed by 2D color TDI and defined as differences between subendocardial and subepicardial velocities (radial MVG) or between basal and apical velocities (longitudinal MVG); OHCM, obstructive hypertrophic cardiomyopathy; PAH, pulmonary arterial hypertension; RA, right atrium; RAE, right atrial enlargement; RV, right ventricle; RVMW, right ventricular myocardial wall; S, peak velocity of systolic pulmonary vein flow; SAM, systolic anterior motion; Sₜᴅɪ, peak myocardial velocity assessed by 2D color TDI during systole; TR, tricuspid regurgitation.
2D、二次元;A、拡張後期僧帽弁流入血流最大速度;Aa、パルス波TDIで評価した拡張後期僧帽弁輪運動最大速度;Adur、僧帽弁A波持続時間;AR、心房収縮時肺静脈逆流最大速度;ARdur、AR波持続時間;Aₜᴅɪ、2DカラーTDIで評価した拡張後期心筋最大速度;D、拡張期肺静脈血流最大速度;DLVOTO、動的左室流出路閉塞;E、拡張早期僧帽弁流入血流最大速度;Ea、パルス波TDIで評価した拡張早期僧帽弁輪運動最大速度;E DT、僧帽弁E波減速時間;EMF、拘束型心筋症の心内膜心筋型;EPSS、E-point-to-septal separation;ES、収縮終期;Eₜᴅɪ、2DカラーTDIで評価した拡張早期心筋最大速度;esp、特に;FS%、短縮率;IVRT、等容性弛緩時間;IVS、心室中隔;LA、左心房;LAE、左房拡大;LV、左心室;LVFP、左室充満圧;LVFW、左室自由壁;LVH、左室肥大;LVOT、左室流出路;MR、僧帽弁逆流;MV、僧帽弁;MVG、2DカラーTDIで評価した心筋速度勾配(心内膜下と心外膜下速度差=放射状MVG、基部と心尖部速度差=縦方向MVG);OHCM、閉塞性肥大型心筋症;PAH、肺動脈高血圧症;RA、右心房;RAE、右房拡大;RV、右心室;RVMW、右室心筋壁;S、収縮期肺静脈血流最大速度;SAM、収縮期前方運動;Sₜᴅɪ、2DカラーTDIで評価した収縮期心筋最大速度;TR、三尖弁逆流。
The definitive diagnosis of primary cardiomyopathy should never be based solely on these imaging criteria. Secondary cardiomyopathies characterized by the same phenotype should always be excluded first.³
原発性心筋症の確定診断は、これらの画像診断基準のみに基づいて行うべきではない。同じ表現型を示す二次性心筋症を常に最初に除外すべきである。³
a Lower cutoff values should be used according to body weight and breeds.³,⁶⁰,⁸⁸ See text for explanation.
a 体重および品種に応じて、より低いカットオフ値を用いるべきである。³,⁶⁰,⁸⁸ 詳細は本文参照。
b Various reference intervals of E DT have been reported (most often <100 ms, but ranging from 45-192 ms, thus rendering this variable less reliable in clinical decision-making).¹⁷,⁷⁴
b E DTの基準範囲にはさまざまな報告があり(多くは<100 msだが、45–192 msまで幅がある)、そのため臨床判断における信頼性はやや低い。¹⁷,⁷⁴
c The lower and upper range of the reference interval for IVRT assessed in 100 healthy awake cats of various breeds was 34 ms and 56 ms, respectively,⁸⁸ with a lower minimal IVRT cut-off value (28 ms) in the Sphynx breed.⁶⁰ An upper IVRT cut-off of 60 ms is often used in practice.⁷⁴
c さまざまな品種の健康な覚醒猫100頭で評価したIVRT基準範囲の下限および上限は、それぞれ34 msおよび56 msであった⁸⁸。スフィンクスではより低いIVRTカットオフ値(28 ms)が報告されている。⁶⁰ 実臨床ではIVRT上限60 msがよく用いられる。⁷⁴
d In late stages of hypertrophic cardiomyopathy, a restrictive pattern (E:A ratio >2 with shortened E DT and IVRT) preceded by a “pseudonormal” pattern may be observed whereas in early stages of restrictive cardiomyopathy, an abnormal relaxation mitral inflow pattern (E:A ratio <1 with prolonged E DT and IVRT) may be found.⁷⁴
d 肥大型心筋症の後期では、“偽正常化”パターンに続いて拘束型パターン(E:A比>2、E DTおよびIVRT短縮)が認められることがある。一方、拘束型心筋症の早期では、異常弛緩型僧帽弁流入パターン(E:A比<1、E DTおよびIVRT延長)が認められる場合がある。⁷⁴
e Unpublished data (personal data; Cardiology Unit of Alfort).
e 未公表データ(個人データ;アルフォール心臓病ユニット)。
The influence of the observer’s experience on the variability of echocardiographic measurements in cats has been demonstrated, with a higher variability for less skilled operators and a frequent tendency of the latter to overestimate myocardial wall thicknesses (up to 2 mm), with a subsequent risk to “overdiagnose” HCM of which practitioners should be aware.¹⁷⁷
猫の心エコー測定値のばらつきには検査者経験が影響することが示されている。熟練度の低い検査者では変動が大きく、心筋壁厚を過大評価(最大2 mm)する傾向があり、その結果HCMを“過剰診断”するリスクがあることに留意すべきである。¹⁷⁷
A breed and body weight effect has been demonstrated for some echocardiographic measurements in cats (e.g., end-diastolic LV diameter, LVFW and IVS thicknesses).⁶⁰,⁸⁸,¹⁷⁸ For example, the end-diastolic cut-off value commonly used to define LVH is ≥6 mm, but lower cut-offs (e.g., 5.0 mm and 5.5 mm) should be used in Sphynx cats weighing <4 kg and ≥4 kg, respectively.⁶⁰
猫の一部心エコー測定値(例:拡張末期左室径、LVFWおよびIVS厚)には品種および体重の影響があることが示されている。⁶⁰,⁸⁸,¹⁷⁸ 例えば、LVHを定義するために一般的に用いられる拡張末期カットオフ値は≥6 mmであるが、スフィンクスでは体重<4 kgで5.0 mm、≥4 kgで5.5 mmなど、より低いカットオフ値を用いるべきである。⁶⁰
LA measurement is of great importance as LAE is considered to be the structural expression of chronicity and severity of diastolic dysfunction in cats with HCM and RCM, with a high prognostic value.⁴⁵,⁶⁸,⁷⁰,⁷⁴ The LA:Ao is commonly used for assessing LAE (Figure 234.9, B), with LA and Ao diameters measured from a right parasternal short-axis view including the aortic cusps. When assessing LA:Ao at end-systole or early diastole (first diastolic frame in which aortic valve closure is evident, when LA is maximal), a LA:Ao >1.5 is consistent with LAE.¹⁷⁹ In the author’s lab, LA:Ao is preferentially assessed at end-diastole (when LA is minimal), as it has been demonstrated to be highly reproducible, with no body weight, breed, or sex effect; it likely more closely reflects the LV end-diastolic pressure than early-systolic measurement (normal values = 0.5-1.2), with a better prognostic value for CHF than maximal LA:Ao in cats with cardiomyopathy.⁷⁴,⁸⁸,¹⁷⁷,¹⁸⁰ Additionally, the LA diameter can be measured parallel to the MV plane, from the middle layer of the atrial septum to the blood-tissue interface of the posterior LA wall, and a diameter of <16 mm is considered normal in most cats. With this method, LAE is categorized as mild (16 mm to <20 mm), moderate (20 mm to <25 mm), or severe (>25 mm).⁷⁴ A systematic subjective evaluation of LA size as compared with other adjacent structures (aorta, atrial septum) is also recommended.⁷⁴ Lastly, in addition to LA size, LA function can be assessed by the LA FS% measured using 2D-guided M-mode from the same parasternal short axis view used for LA:Ao measurement.³,¹⁷⁹
左房計測は非常に重要である。なぜなら、LAEはHCMおよびRCM猫における拡張機能障害の慢性度および重症度を構造的に反映する所見であり、高い予後予測価値を有するためである。⁴⁵,⁶⁸,⁷⁰,⁷⁴ LAE評価には一般的にLA:Ao比(図234.9B)が用いられ、大動脈弁尖を含む右傍胸骨短軸像でLA径およびAo径を測定する。収縮終期または拡張早期(大動脈弁閉鎖が確認できる最初の拡張期フレームで、LA最大時)にLA:Aoを評価した場合、LA:Ao >1.5 はLAEと一致する。¹⁷⁹ 著者らの施設では、再現性が高く、体重・品種・性別の影響を受けず、また早期収縮期測定より左室拡張末期圧をよりよく反映すると考えられるため、LA最小時である拡張末期でのLA:Ao測定を優先している(正常値0.5–1.2)。さらに、この測定は心筋症猫において最大LA:AoよりもCHF予後予測価値に優れる。⁷⁴,⁸⁸,¹⁷⁷,¹⁸⁰ 加えて、LA径はMV平面に平行に、心房中隔中央層から後方LA壁の血液‐組織境界まで測定可能であり、多くの猫では<16 mmが正常とされる。この方法ではLAEを軽度(16 mm〜<20 mm)、中等度(20 mm〜<25 mm)、重度(>25 mm)に分類する。⁷⁴ また、他の隣接構造(大動脈、心房中隔)と比較した体系的主観評価も推奨される。⁷⁴ 最後に、LAサイズに加えて、LA機能はLA:Ao測定と同じ右傍胸骨短軸像から2DガイドMモードで測定したLA FS%によって評価可能である。³,¹⁷⁹
Tissue Doppler Imaging for Assessment of Myocardial Motion (Table 234.4):心筋運動評価のための組織ドプライメージング(Table 234.4)
TDI quantifies myocardial velocities in real time and offers a sensitive and quantitative analysis of regional myocardial function (Video 234.1).¹⁸¹˒¹⁸² Several studies have demonstrated the ability of 2D color TDI to analyze LV myocardial function in awake healthy cats⁸⁸˒¹⁸² and in awake cats with HCM.⁴¹˒⁴² Other TDI modes (pulsed-wave mode and color M-mode) may also be used, although velocity measurements are then limited to a single segment or line, respectively, which decreases the diagnostic abilities of the technique.⁷¹˒⁷²˒⁸⁰ Another drawback of the pulsed-wave TDI mode is the inability to change the position and size of the region of interest within the myocardium with post-processing. Nevertheless, pulsed-wave TDI is commonly used in cats to assess Ea, which allows E:Ea to be calculated (see above; Figure 234.9,E).⁷⁴
TDIは、リアルタイムで心筋速度を定量化し、局所心筋機能の高感度かつ定量的解析を可能にする(Video 234.1)。¹⁸¹˒¹⁸²複数の研究により、2DカラーTDIが、覚醒下正常猫⁸⁸˒¹⁸²および覚醒下HCM猫⁴¹˒⁴²におけるLV心筋機能解析に有用であることが示されている。他のTDIモード(パルス波モードおよびカラーMモード)も利用可能であるが、それぞれ単一セグメントまたは単一ラインに測定が限定されるため、診断能は低下する。⁷¹˒⁷²˒⁸⁰パルス波TDIモードのもう一つの欠点は、後処理によって心筋内の関心領域の位置やサイズを変更できないことである。それにもかかわらず、パルス波TDIは猫においてEa評価に一般的に用いられており、これによってE:Ea比を算出できる(前述;Figure 234.9,E)。⁷⁴
Radial and longitudinal diastolic LVFW and IVS motions assessed by 2D color TDI are similarly altered in cats with HCM (Videos 234.17, 234.18) and in cats with LVH due to systemic arterial hypertension.⁴¹ Longitudinal regional systolic dysfunction is an additional component of HCM-associated myocardial alteration. The abnormality consists of a decrease in systolic myocardial velocities and gradients as well as TDI systolic strain despite normal or increased LV FS%.⁴¹˒¹⁸³ Most importantly, 2D color TDI has been shown to be more sensitive than conventional echocardiography for detecting regional myocardial dysfunction in both feline HCM and a feline HCM model, before the occurrence of or in the absence of overt myocardial hypertrophy.⁴¹˒⁴²˒⁷³˒¹⁵⁵ However, it is important to emphasize that to optimize the abilities of TDI to detect myocardial dysfunction early, the 2D color TDI mode should be preferred for the aforementioned reasons, cats should not be sedated, and the use of summated early and late diastolic velocities should be avoided. As performed in the author’s lab, calm animal handling in a relaxing environment and with minimal restraint by performing ultrasound examinations with the cat standing is highly recommended to reduce stress, thus avoiding fusion of diastolic waves in about 90% of cats.⁷⁴˒⁸⁸ The TDI technique is also commonly used for differentiating constrictive pericarditis from RCM in humans.¹⁸⁴ However, TDI data on feline RCM are currently lacking.
2DカラーTDIによって評価される放射方向および長軸方向の拡張期LV自由壁(LVFW)および心室中隔(IVS)運動は、HCM猫(Videos 234.17、234.18)および全身性動脈性高血圧に起因するLVH猫において同様に異常を示す。⁴¹長軸方向局所収縮機能障害は、HCM関連心筋異常の追加的構成要素である。この異常は、LV FS%が正常または増加しているにもかかわらず、収縮期心筋速度および速度勾配、さらにTDI収縮期ストレインが低下することで特徴づけられる。⁴¹˒¹⁸³最も重要な点として、2DカラーTDIは、通常の心エコー検査よりも高感度に、猫HCMおよび猫HCMモデルにおける局所心筋機能障害を検出できることが示されており、明らかな心筋肥大が出現する以前、あるいは存在しない段階でも異常を検出可能である。⁴¹˒⁴²˒⁷³˒¹⁵⁵しかしながら、TDIによる早期心筋機能障害検出能を最大化するためには、上述の理由から2DカラーTDIモードを優先すべきであり、猫は鎮静すべきではなく、また早期および後期拡張期速度の加算値の使用は避けるべきであることを強調する必要がある。著者らの研究室で行われているように、リラックスした環境下で穏やかに動物を扱い、猫を立位のまま最小限の保定で超音波検査を行うことは、ストレスを軽減し、その結果として約90%の猫で拡張期波形融合を回避できるため、強く推奨される。⁷⁴˒⁸⁸TDI技術は、人において収縮性心膜炎とRCMを鑑別するためにも一般的に用いられている。¹⁸⁴しかし、猫RCMに関するTDIデータは現在不足している。
CARDIAC MAGNETIC RESONANCE IMAGING:心臓MRI
Cardiac magnetic resonance imaging (cMRI) has emerged as a powerful tool in human patients with cardiomyopathies, providing data on cardiac volumes and function and on tissue characterization (fibrosis and fatty infiltration). In Maine Coon cats with moderate to severe HCM, no difference in cMRI indices of diastolic function was found compared to control cats, while echocardiographic TDI could detect diastolic dysfunction in all HCM cats.¹⁸⁵⁻¹⁸⁷
心臓MRI(cMRI)は、人の心筋症症例において強力な診断ツールとして登場しており、心臓容積、機能、および組織特性(線維化や脂肪浸潤)に関する情報を提供する。中等度から重度HCMを有するメインクーン猫では、対照猫と比較してcMRIによる拡張機能指標に差は認められなかった一方で、心エコーTDIはすべてのHCM猫において拡張機能障害を検出可能であった。¹⁸⁵⁻¹⁸⁷
OTHER DIAGNOSTIC TOOLS:その他の診断ツール
Electrocardiography:心電図検査
As described above, various arrhythmias and nonspecific morphological ECG alterations are associated with feline myocardial diseases. However, the sensitivity of 6-lead ECG to predict LVH and LAE enlargement in cats is low, and therefore ECG is currently not recommended for screening cats for HCM.³˒⁸⁴˒¹⁸⁸ Conversely, ECG and, if necessary, 24-hour Holter monitoring (which is more sensitive than “in-clinic” ECG for arrhythmia detection) are recommended for cats demonstrating syncope, weakness, or seizures of unknown origin.³˒⁸⁵˒⁸⁷ As some cats may not tolerate Holter monitoring well, event monitors and portable owner-operated ECG devices connected to smartphones or tablets (e.g., Kardia Alivecor) are other possible options for ECG tracing recording in the cat’s home environment (ch. 96).³
前述の通り、さまざまな不整脈および非特異的形態学的ECG異常が猫の心筋疾患に関連している。しかし、6誘導ECGによるLVHおよびLAE予測感度は低く、そのため現在、ECGは猫HCMスクリーニングには推奨されていない。³˒⁸⁴˒¹⁸⁸一方で、失神、虚弱、または原因不明の痙攣発作を示す猫では、ECGおよび必要に応じて24時間Holterモニタリング(不整脈検出において院内ECGより高感度)が推奨される。³˒⁸⁵˒⁸⁷一部の猫ではHolterモニタリングへの耐容性が低いため、イベントモニターや、スマートフォンまたはタブレットと接続した飼い主操作型携帯ECG装置(例:Kardia Alivecor)も、自宅環境でのECG記録の選択肢となり得る(第96章)。³
Genetic Tests:遺伝子検査
Genetic tests performed on blood or buccal swab samples are currently available to identify the MyBPC3-A31P and MyBPC3 R820W mutations in Maine Coon and Ragdoll cats, respectively. These tests are recommended for cats from these two breeds when the cats are intended for breeding. Cats that are homozygous for either mutation should be excluded from breeding programs (heterozygous cats also, with the rare exception for those with outstanding features and only if bred to a homozygous-wild genotype cat).³ These genetic tests can also be used for determining the relative risk of a given Maine Coon or Ragdoll cat developing and dying from HCM (see above). Importantly, these tests are not recommended for non-Maine Coon cats and non-Ragdoll cats, as the mutations appear to be almost completely breed-specific.³˒⁵²˒⁵³
現在、血液または口腔スワブサンプルを用いた遺伝子検査によって、メインクーン猫およびラグドール猫におけるそれぞれMyBPC3-A31P変異およびMyBPC3 R820W変異を同定可能である。これらの検査は、繁殖目的のこれら2品種の猫に推奨される。いずれかの変異に対してホモ接合体である猫は繁殖計画から除外すべきであり、ヘテロ接合体猫も同様である。ただし、極めて優れた特徴を持ち、かつホモ接合野生型遺伝子型の猫との交配に限る場合は例外とされる。³これらの遺伝子検査は、特定のメインクーン猫またはラグドール猫がHCMを発症し死亡する相対的リスクの評価にも利用可能である(前述参照)。重要な点として、これらの変異はほぼ完全に品種特異的であるため、非メインクーン猫および非ラグドール猫にはこれらの検査は推奨されない。³˒⁵²˒⁵³
Biomarkers (Cardiac Troponins and NT-proBNP)¹⁸⁹⁻²⁰¹:バイオマーカー(心筋トロポニンおよびNT-proBNP)¹⁸⁹⁻²⁰¹
Circulating cardiac troponin I and T concentrations (cTnI, cTnT) are highly sensitive and specific indicators of acute myocardial cell injury independent of the underlying cause. The circulating cardiac troponin concentration should be assayed in cases of echocardiographic suspicion of myocardial infarction, a rare complication of HCM.³³˒¹³⁷ Feline HCM is associated with elevated circulating cTnI and cTnT concentrations, with cTnI revealing a higher percentage of cats with myocardial injury (67%) than cTnT (28%).¹⁸⁹ Using high-sensitivity cTnI assays, plasma cTnI concentration has been shown to reflect HCM severity and to be a predictor of cardiac death in cats with HCM (cutoff >0.7 ng/mL) independently of the presence of CHF or LAE.¹⁹⁰˒¹⁹¹ Additionally, a cutoff of 0.06 ng/mL was demonstrated to provide good discrimination between healthy cats and cats with HCM (sensitivity, 91.7%; specificity, 95.4%), even for cats with ACVIM stage B HCM (sensitivity and specificity of 87.8% and 95.4%, respectively). These results suggest that circulating cTnI concentrations may help differentiate normal cats from cats with subclinical HCM.¹⁹²
循環中の心筋トロポニンIおよびT濃度(cTnI、cTnT)は、基礎疾患に関係なく、急性心筋細胞障害に対する高感度かつ高特異度の指標である。循環心筋トロポニン濃度は、HCMの稀な合併症である心筋梗塞が心エコー検査で疑われる場合に測定すべきである。³³˒¹³⁷猫HCMでは循環cTnIおよびcTnT濃度の上昇が認められ、cTnIはcTnTよりも高率に心筋障害猫を検出した(67%対28%)。¹⁸⁹高感度cTnI測定法を用いた場合、血漿cTnI濃度はHCM重症度を反映し、CHFまたはLAEの有無とは独立して、HCM猫における心臓死予測因子となることが示されている(cutoff >0.7 ng/mL)。¹⁹⁰˒¹⁹¹さらに、0.06 ng/mLというcutoff値は、健康猫とHCM猫を良好に識別できることが示されており(感度91.7%、特異度95.4%)、ACVIM stage B HCM猫においても有用であった(感度87.8%、特異度95.4%)。これらの結果は、循環cTnI濃度が正常猫と無症候性HCM猫の鑑別に役立つ可能性を示唆している。¹⁹²
Plasma N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentration, which primarily increases in response to myocardial wall stress, can distinguish CHF from primary respiratory diseases in dyspneic cats with approximately 90% diagnostic accuracy. Its use in addition to conventional diagnostic tests significantly increases the accuracy of differential diagnosis for general practitioners.¹⁹⁵˒¹⁹⁶ NT-proBNP concentration can be measured in pleural fluid samples, which differentiates cardiac from non-cardiac pleural effusion with also good diagnostic accuracy (sensitivity = 100%; specificity, 76.5%).¹⁹⁷ However, in emergency conditions requiring immediate decisions (e.g., cats with acute dyspnea), NT-proBNP point-of-care tests should be preferred to quantitative NT-proBNP assays because they provide rapid results. This may be particularly useful to differentiate cardiac from non-cardiac causes of respiratory distress when point-of-care ultrasound examination is not available.¹⁷⁴˒¹⁹⁷˒¹⁹⁸ Samples for NT-proBNP point-of-care testing can be feline plasma or feline pleural effusion fluid; the latter should be diluted 1:1 with 0.9% NaCl for greater specificity.¹⁹⁸
血漿N-terminal pro-B-type natriuretic peptide(NT-proBNP)濃度は、主として心筋壁ストレスに応答して増加し、呼吸困難を示す猫において、約90%の診断精度でCHFと原発性呼吸器疾患を鑑別可能である。従来の診断検査に加えてNT-proBNPを用いることで、一般臨床医における鑑別診断精度は有意に向上する。¹⁹⁵˒¹⁹⁶NT-proBNP濃度は胸水サンプルでも測定可能であり、心原性胸水と非心原性胸水を良好な診断精度(感度100%、特異度76.5%)で鑑別できる。¹⁹⁷しかし、迅速な意思決定が必要な緊急状況(急性呼吸困難猫など)では、迅速な結果が得られるため、定量的NT-proBNP測定よりもpoint-of-care NT-proBNP検査が推奨される。これは、point-of-care超音波検査が利用できない場合に、呼吸困難の心原性・非心原性鑑別に特に有用である可能性がある。¹⁷⁴˒¹⁹⁷˒¹⁹⁸NT-proBNP point-of-care検査には猫血漿または猫胸水を使用可能であり、後者では特異度向上のため0.9% NaClで1:1に希釈すべきである。¹⁹⁸
Plasma NT-proBNP also may help in discriminating healthy cats from cats with occult cardiomyopathy (specificity and sensitivity of 100% and 70.8%, respectively for a >99 pmol/L cut-off, with a positive correlation between NT-proBNP and LV thicknesses or LA:Ao ratio).¹⁹³˒¹⁹⁹ However, the quantitative NT-proBNP assay is not recommended to differentiate healthy cats from cats with mild to moderate HCM.³ Similarly, using NT-proBNP point-of-care testing in apparently healthy cats, positive results are highly suggestive of moderate to severe occult heart disease (which needs to be further confirmed by echocardiography), whereas negative results cannot differentiate normal cats from those with mild occult heart disease.²⁰⁰˒²⁰¹
血漿NT-proBNPは、健常猫と潜在性心筋症猫の鑑別にも役立つ可能性があり、>99 pmol/L cutoffにおける特異度および感度はそれぞれ100%および70.8%であり、NT-proBNPとLV壁厚またはLA:Ao比との正の相関が認められている。¹⁹³˒¹⁹⁹しかし、定量的NT-proBNP測定は、健康猫と軽度〜中等度HCM猫との鑑別には推奨されない。³同様に、見かけ上健康な猫におけるNT-proBNP point-of-care検査では、陽性結果は中等度〜重度潜在性心疾患を強く示唆するが(さらなる心エコー検査による確認が必要)、陰性結果では正常猫と軽度潜在性心疾患猫を鑑別できない。²⁰⁰˒²⁰¹
MANAGEMENT:管理
Few prospective randomized controlled clinical trials (PRCCTs) are reported in cats with heart disease. The ACVIM Consensus Statement proposes recommendations for treating feline cardiomyopathies based on 3 levels of evidence (LOE): high (randomized controlled trials or prospective nonrandomized with adequate methodology in cats), medium (experimental trials in cats or retrospective clinical studies with control groups), and low (case series without control groups, study in other species, expert opinion).³ The medications used for treating cats with cardiomyopathies are presented in Table 234.5.
猫の心疾患に関する前向き無作為化比較臨床試験(PRCCTs)は少ない。ACVIMコンセンサスステートメントでは、3段階のエビデンスレベル(LOE)に基づいた猫心筋症治療推奨を提示している。すなわち、高(猫における無作為化比較試験、または適切な方法論を有する前向き非無作為化試験)、中(猫における実験的試験、または対照群を有する後ろ向き臨床研究)、低(対照群を持たない症例集積、他種での研究、専門家意見)である。³猫心筋症治療に用いられる薬剤はTable 234.5に示されている。
TABLE 234.5 Drugs Most Commonly Used for Treatment of Feline Cardiomyopathies³
表234.5 猫の心筋症治療で最も一般的に使用される薬剤³
| DRUG CATEGORY AND NAME 薬剤分類および薬剤名 | PHARMACOLOGICAL ACTION OF INTEREST 注目される薬理作用 | REPORTED DOSAGES AND ROUTES 報告されている用量および投与経路 | INDICATIONS 適応 | CONTRAINDICATIONS 禁忌 | POTENTIAL SIDE-EFFECTS 潜在的副作用 | ADVICE – COMMENTS 助言・コメント | |
|---|---|---|---|---|---|---|---|
|
Aldosterone antagonist アルドステロン拮抗薬 Spironolactone スピロノラクトン |
Selective aldosterone receptor antagonist; thus K-sparing diuretic, potential ↓ cardiac remodeling & hypertrophy 選択的アルドステロン受容体拮抗薬;したがってカリウム保持性利尿薬であり、心リモデリングおよび肥大抑制作用の可能性を有する |
0.5-3 mg/kg PO q24h or 0.5-1.5 mg/kg PO q12h |
CHF refractory to standard therapy (ACVIM stage D) 標準治療抵抗性CHF(ACVIMステージD) |
Hyperkalemia 高カリウム血症 |
Ulcerative facial dermatitis reported at 2 mg/kg PO q12h 2 mg/kg PO q12hで潰瘍性顔面皮膚炎の報告あり |
Monitor blood renal parameters and electrolyte concentrations 腎パラメータおよび電解質濃度をモニターする | |
|
Drugs used as anti-arrhythmic agents 抗不整脈薬 |
Digoxin ジゴキシン |
Antiarrhythmic properties with mild positive inotropic action 軽度陽性変力作用を伴う抗不整脈作用 |
0.007 mg/kg PO q48h or one-fourth of a 0.125 mg tablet PO q12-24h (cats >6 kg), q24h (cats 3-6 kg), or q48h (cats <3 kg) |
• SVTs including AF • Myocardial failure (e.g., DCM) • AFを含む上室性頻拍 • 心筋機能不全(例:DCM) |
Ventricular tachyarrhythmias 心室頻脈性不整脈 |
• Anorexia • Vomiting • Arrhythmias (ventricular arrhythmias, bradycardia, AV block) • ↑ toxicity with hypokalemia • 食欲不振 • 嘔吐 • 不整脈(心室性不整脈、徐脈、房室ブロック) • 低カリウム血症で毒性増加 |
• Steady-state concentrations reached in 8-10 days but variable half-life • Serum concentration checked 8 h post-pill after 8-10 days of treatment • Therapeutic range = 0.7-2 ng/mL • Avoid in cats with renal dz • 定常状態到達まで8-10日を要するが半減期は変動する • 血中濃度は治療8-10日後、投与8時間後に測定 • 治療域 = 0.7-2 ng/mL • 腎疾患猫では回避 |
|
Diltiazem ジルチアゼム |
See below (calcium channel blockers) 下記参照(カルシウムチャネル遮断薬) | ||||||
|
Esmolol エスモロール |
Short-acting beta-blocker 短時間作用型β遮断薬 | Loading dose 50-500 mcg/kg slow IV bolus over 1-2 minutes, then IV CRI 10-200 mcg/kg/min |
Acute management of SVTs, ventricular tachyarrhythmias refractory to lidocaine SVTおよびリドカイン抵抗性心室頻脈性不整脈の急性管理 |
• Hypotension • Severe myocardial failure • 低血圧 • 重度心筋不全 |
• Arrhythmias (bradycardia, AV block) • Systemic hypotension • Negative inotropic effect • 不整脈(徐脈、房室ブロック) • 全身性低血圧 • 陰性変力作用 |
Start with lowest dosages if myocardial failure (to be confirmed by echo) 心筋不全がある場合(心エコーで確認)は最低用量から開始 | |
|
Ivabradine イバブラジン |
Selective SA nodal funny current (If) inhibitor (negative chronotrope) 洞結節funny current(If)選択的阻害薬(陰性変時作用) | 0.3 mg/kg PO q12h |
Sinus tachycardia 洞性頻脈 |
Bradycardia 徐脈 | |||
|
Lidocaine リドカイン |
Class Ib antiarrhythmic クラスIb抗不整脈薬 | 0.2-0.5 mg/kg slow IV bolus over 5 minutes, repeat 1-2 times only, followed by not by 10-30 mcg/kg/min IV CRI |
Initial emergency treatment of ventricular tachyarrhythmias 心室頻脈性不整脈の初期救急治療 |
• Hypotension • Severe myocardial failure • 低血圧 • 重度心筋不全 |
• Arrhythmias (bradycardia, AV block) • CNS toxicosis (e.g., muscle tremors, seizures; controlled with diazepam) • 不整脈(徐脈、房室ブロック) • 中枢神経毒性(例:筋振戦、痙攣;ジアゼパムで制御) |
• Use cautiously due to risk of seizures • Start with lowest dosage if myocardial failure (to be confirmed by echo) • Monitor serum K+ (↑ K+ intensifies EP effects; ↓ K+ decreases them) • 痙攣リスクのため慎重使用 • 心筋不全時は最低用量から開始(心エコー確認) • 血清K+をモニター(高K+は電気生理作用増強、低K+は減弱) | |
|
Sotalol ソタロール |
Beta-blocker with class III antiarrhythmic properties クラスIII抗不整脈作用を有するβ遮断薬 |
10-20 mg/cat PO q12h or 2 mg/kg PO q12h |
• Chronic oral treatment of ventricular tachyarrhythmias • May be considered for AF (rate control) • 心室頻脈性不整脈の慢性経口治療 • AFのレートコントロールとして考慮可能 |
• Hypotension • Severe myocardial failure • 低血圧 • 重度心筋不全 |
• Bradycardia • Systemic hypotension • Negative inotropic effect • Anorexia • Weakness, depression • 徐脈 • 全身性低血圧 • 陰性変力作用 • 食欲不振 • 脱力、抑うつ |
• Decrease dosage if renal dz • Start with lowest dosage if myocardial failure (to be confirmed by echo) and/or CHF • Monitor myocardial function (echo) • 腎疾患では減量 • 心筋不全および/またはCHFでは最低用量から開始(心エコー確認) • 心筋機能をモニター(心エコー) |
| DRUG CATEGORY AND NAME 薬剤分類および薬剤名 | PHARMACOLOGICAL ACTION OF INTEREST 注目される薬理作用 | REPORTED DOSAGES AND ROUTES 報告されている用量および投与経路 | INDICATIONS 適応 | CONTRAINDICATIONS 禁忌 | POTENTIAL SIDE-EFFECTS 潜在的副作用 | ADVICE – COMMENTS 助言・コメント | |
|---|---|---|---|---|---|---|---|
|
Antithrombotic drugs 抗血栓薬 |
Aspirin アスピリン |
Nonsteroidal anti-inflammatory that inhibits platelet aggregation 血小板凝集を抑制する非ステロイド性抗炎症薬 | 5-81 mg/cat PO q72h or 5 mg/cat to 5 mg/kg PO q72h, administered with food |
Prevention of ATE ATE予防 |
• Dehydration • Hypotension • GI signs • Bleeding disorders • 脱水 • 低血圧 • 消化器症状 • 出血性疾患 |
• Anorexia, hematemesis/vomiting (GI ulceration risk) • Bleeding (at higher dosages and/or in combination with other antithrombotics) • 食欲不振、吐血/嘔吐(消化管潰瘍リスク) • 出血(高用量時および/または他の抗血栓薬併用時) |
• ↓ risk of adverse effects at lowest dosages • Lower ATE prophylactic effects than clopidogrel (ch. 238) • 最低用量で副作用リスク低下 • ATE予防効果はクロピドグレルより低い(第238章) |
|
Clopidogrel クロピドグレル |
Thienopyridine derivative (inhibits ADP-mediated platelet aggregation) チエノピリジン誘導体(ADP依存性血小板凝集抑制) | 18.75 mg/cat PO q24h with foodᵃ |
First line treatment for prevention of ATE ATE予防の第一選択治療 |
• GI signs • Bleeding disorders • 消化器症状 • 出血性疾患 |
Salivation, anorexia, vomiting, diarrhea 流涎、食欲不振、嘔吐、下痢 |
• First line treatment in cats at risk of ATEᵇ • ATEリスク猫における第一選択治療ᵇ | |
|
Rivaroxaban リバーロキサバン |
• Direct oral anticoagulant (factor Xa inhibitor) • 直接経口抗凝固薬(Xa因子阻害薬) |
• 2.5 mg/cat PO q24h or • 0.5-1 mg/kg PO q24h |
• Treatment of recurrent ATE • 再発性ATEの治療 |
• Bleeding disorders • 出血性疾患 |
• Sparsely documented to date in cats; bleeding • 猫での報告はまだ少ないが、出血あり |
• Added to, or given instead of, clopidogrel in high-risk, treatment-resistant ATE • 高リスク・治療抵抗性ATEではクロピドグレル追加または代替として使用 | |
|
ACE inhibitors ACE阻害薬 |
Benazepril ベナゼプリル |
• RAAS inhibitor; thus, vasodilation (↓ ventricular preload and afterload), myocardial ischemia, ↓ water and Na+ retention, potential ↓ cardiac remodeling and hypertrophy • Renal protective effect • RAAS阻害薬;したがって血管拡張(心室前負荷・後負荷低下)、心筋虚血軽減、水分・Na+貯留低下、心リモデリングおよび肥大抑制の可能性 • 腎保護作用 | 0.25-0.5 mg/kg PO q12-24h |
• CHF (co-treatment with furosemide) • Myocardial remodeling associated with HCM and RCM • CHF(フロセミド併用) • HCMおよびRCMに関連する心筋リモデリング |
• Dehydration • Oliguria/anuria (acute renal failure) • Hypotension • 脱水 • 乏尿/無尿(急性腎不全) • 低血圧 |
Usually safe, but possible side-effects: • Hypotension (esp. if OHCM, severe myocardial failure) • Prerenal azotemia if dehydration and/or high furosemide dosage 通常安全だが、副作用の可能性あり: • 低血圧(特にOHCM、重度心筋不全) • 脱水および/または高用量フロセミド時の腎前性高窒素血症 |
• Monitor hydration • Monitor BP, esp if OHCM, myocardial failure (“start with one-fourth to one-half dose); if hypotension, administer q12h • Monitor renal function, electrolytes • Imidapril: oral liquid licensed for dogs, practical for use in some cats; good tolerance at very high dosage • Discontinue if dehydration and/or anorexia and/or oliguria/anuria • 水和状態をモニター • 血圧をモニター(特にOHCM、心筋不全では通常量の1/4〜1/2で開始);低血圧ならq12h投与 • 腎機能・電解質をモニター • イミダプリル:犬用液剤あり。一部猫で実用的、高用量耐容性良好 • 脱水、食欲不振、乏尿/無尿時は中止 |
|
Enalapril エナラプリル | 0.25-0.5 mg/kg PO q12-24 h | ||||||
|
Imidapril イミダプリル | 0.25-0.5 mg/kg PO q24 h (dosage if given with food) | ||||||
|
Ramipril ラミプリル | 0.25-0.5 mg/kg PO q24 h | ||||||
|
Beta-blocker (other than esmolol and sotalol) β遮断薬(エスモロールおよびソタロール以外) |
Atenolol アテノロール |
Beta-blocker (beta-1 selective): • ↓ diastolic function via ↓ inotropy (= also LVOTO) and chronotropy • Antiarrhythmic properties (SVTs, ventricular tachyarrhythmias) β遮断薬(β1選択的): • 陰性変力・陰性変時作用による拡張機能低下(LVOTOも低下) • 抗不整脈作用(SVT、心室頻脈性不整脈) |
6.25-12.5 mg/cat PO q12-24h or 0.2-1 (2) mg/kg q24h |
• ACVIM stage B HCM with severe dynamic LVOTO • Ventricular tachyarrhythmias • May be considered for AF (rate control) • 重度動的LVOTOを伴うACVIM stage B HCM • 心室頻脈性不整脈 • AFのレートコントロールに考慮可能 |
Severe myocardial failure 重度心筋不全 |
• Arrhythmias (bradycardia, AV block) • Hypotension • Weakness • Depression • 不整脈(徐脈、房室ブロック) • 低血圧 • 脱力 • 抑うつ |
• Should not be started in cats with CHF • Perform echo before prescription to confirm absence of ↓ systolic function • Begin with lowest dosage • Gradual taper if discontinuing • CHF猫では開始すべきでない • 処方前に心エコーで収縮機能低下がないことを確認 • 最低用量から開始 • 中止時は漸減 |
|
Calcium channel blockers (benzothiazepine) カルシウムチャネル遮断薬(ベンゾチアゼピン系) |
Diltiazem ジルチアゼム |
• Improves diastolic function through ↓ inotropy and chronotropy, and coronary arteriolar dilation • Directly improves relaxation • Antiarrhythmic properties • 陰性変力・陰性変時作用および冠動脈細動脈拡張により拡張機能改善 • 弛緩を直接改善 • 抗不整脈作用 |
• 1-3 mg/kg PO q8h • For emergency treatment of SVTs: 0.05-0.25 mg/kg slow IV bolus over 2 minutes (can repeat 15 minutes later), then 2-6 mg/kg/min IV CRI |
• Diastolic dysfunction (HCM, RCM) • SVTs including AF • 拡張機能障害(HCM、RCM) • AFを含むSVT |
• Bradycardia • AV block • Hypotension • Hepatopathy • Myocardial failure (e.g., DCM) • 徐脈 • 房室ブロック • 低血圧 • 肝障害 • 心筋不全(例:DCM) |
Usually well tolerated but at highest dosages: • Hypotension • Anorexia, lethargy, esp. if beginning at high dosage • Rare skin reactions and GI signs (esp. extended-release) • Bradycardia, AV blocks 通常は良好に耐容されるが高用量では: • 低血圧 • 食欲不振、嗜眠(特に高用量開始時) • 稀な皮膚反応および消化器症状(特に徐放製剤) • 徐脈、房室ブロック |
• Echocardiography before prescription to confirm absence of decreased systolic function • Extended-release formulation: 5-10 mg/cat PO q24h • 処方前に心エコーで収縮機能低下がないことを確認 • 徐放製剤:5-10 mg/cat PO q24h |
|
Diuretics 利尿薬 |
Furosemide フロセミド |
Loop diuretic (high potency diuretic effect) ループ利尿薬(高力価利尿作用) |
• Emergency: 1-4 mg/kg IV/IM/SC; response (RR) dictates interdose interval; max. 8 mg/kg/day • Chronic: usually 0.5-2 mg/kg PO q8-24h |
CHF (first line treatment) CHF(第一選択治療) |
Stage B cardiomyopathy with normal atrial dimensions 心房径正常のStage B心筋症 |
• Hypo-, hyperNa+, hypoNa+, metabolic alkalosis • Azotemia • Dehydration, hypotension • Lethargy • 低Na+/高Na+、代謝性アルカローシス • 高窒素血症 • 脱水、低血圧 • 嗜眠 |
• Find the lowest effective dosage • Decreased oral absorption in advanced CHF (switch some PO doses to SC) • Monitor hydration, renal parameters, blood electrolytes • 最低有効量を見つける • 進行CHFでは経口吸収低下(POの一部をSCへ変更) • 水和状態、腎パラメータ、血中電解質をモニター |
|
Hydrochlorothiazide ヒドロクロロチアジド |
• Thiazide diuretic • サイアザイド系利尿薬 | • 0.5-2 mg/kg PO q12-24h |
• CHF refractory to furosemide, in combination with furosemide • (ACVIM stage D) • フロセミド抵抗性CHF(フロセミド併用) • (ACVIM stage D) |
• Same as furosemide • フロセミドと同様 |
• Same as furosemide • フロセミドと同様 |
• Find the lowest effective dosage • Monitor hydration, renal parameters, blood electrolytes • 最低有効量を見つける • 水和状態、腎パラメータ、血中電解質をモニター | |
|
Torsemide/torasemide トルセミド |
• Loop diuretic (↑ potency and duration of action compared to furosemide) • ループ利尿薬(フロセミドより高力価・長時間作用) |
• Recommended instead of furosemide when CHF persists despite furosemide >6 mg/kg/day. • Starting dosage: 0.1-0.2 mg/kg PO q24h, uptitrating to effect |
• CHF refractory to furosemide (ACVIM stage D) • フロセミド抵抗性CHF(ACVIM stage D) |
• Same as furosemide • フロセミドと同様 |
• Find the lowest effective dosage • Monitor hydration, renal parameters, blood electrolytes • One-third of cats with CHF also require a dose of furosemide 12 h after torsemide • 最低有効量を見つける • 水和状態、腎パラメータ、血中電解質をモニター • CHF猫の約1/3ではトルセミド12時間後にフロセミド追加が必要 |
| DRUG CATEGORY AND NAME 薬剤分類および薬剤名 | PHARMACOLOGICAL ACTION OF INTEREST 注目される薬理作用 | REPORTED DOSAGES AND ROUTES 報告されている用量および投与経路 | INDICATIONS 適応 | CONTRAINDICATIONS 禁忌 | POTENTIAL SIDE-EFFECTS 潜在的副作用 | ADVICE – COMMENTS 助言・コメント | |
|---|---|---|---|---|---|---|---|
|
Inotropes 強心薬 |
Dobutamine ドブタミン |
Adrenergic agonist (positive inotrope) アドレナリン作動薬(陽性変力作用) | 1-5 mcg/kg/min IV CRI (start at minimal dosage and uptitrate to desired effect) |
Acute management of CHF with ↓ CO (if no improvement with pimobendan) 心拍出量低下を伴うCHFの急性管理(ピモベンダンで改善しない場合) |
Severe ventricular tachyarrhythmias 重度心室頻脈性不整脈 |
• Tachyarrhythmias • Seizures • HypoK+ (prolonged use) • ↑ myocardial O₂ demand • 頻脈性不整脈 • 発作 • 低カリウム血症(長期使用) • 心筋酸素需要増加 |
Use with caution (monitor BP, ECG during administration) 慎重に使用(投与中は血圧・ECGをモニター) |
|
Pimobendan ピモベンダン |
Inodilator (calcium sensitizer, PDE III inhibitor) イノダイレーター(カルシウム感受性増強薬、PDE III阻害薬) | 0.1-0.3 mg/kg PO q12h or 0.625-1.25 mg/cat PO q12h; ≥1 h before food |
• Acute CHF with ↓ CO (e.g., ↓ BP, hypothermia, bradycardia) • DCM • Systolic dysfunction as complication of any CM except OHCM • CHF refractory to standard therapy • 心拍出量低下を伴う急性CHF(例:低血圧、低体温、徐脈) • DCM • OHCM以外のCMに伴う収縮機能障害 • 標準治療抵抗性CHF |
Clinically relevant LVOTO 臨床的に重要なLVOTO |
• Agitation • Hypotension in cases of OHCM • 興奮 • OHCM症例での低血圧 |
Echo before prescription to exclude dynamic LVOTO (OHCM) and confirm myocardial failure 処方前に心エコーで動的LVOTO(OHCM)を除外し、心筋不全を確認 | |
|
Sedative/analgesic 鎮静薬/鎮痛薬 |
Butorphanol ブトルファノール |
Synthetically-derived opiate kappa agonist/mu opioid antagonist 合成オピオイドκ受容体作動薬/μオピオイド拮抗薬 | 0.1-0.4 mg/kg slow IV or IM (repeat if needed q1-4h) |
Decreased stress (acute CHF) ストレス軽減(急性CHF) |
Depressed animals 抑うつ状態の動物 |
• Lethargy • Depression • 嗜眠 • 抑うつ | |
|
Taurine タウリン |
2-aminoethanesulfonic acid (sulfonic acid) 2-アミノエタンスルホン酸(スルホン酸) | 250-500 mg/cat PO q12h |
• Taurine-deficient myocardial failure • DCM • Systolic dysfunction as complication of any other CM • タウリン欠乏性心筋不全 • DCM • その他CMに伴う収縮機能障害 |
If taurine-deficient myocardial failure: clinical improvement in 1-2 weeks, echo improvement in 3-9 weeksᵉ タウリン欠乏性心筋不全では、1-2週間で臨床改善、3-9週間で心エコー改善ᵉ |
うっ血性心不全治療薬の追加情報は第229章、不整脈治療薬については第230章、大動脈血栓塞栓症治療薬については第238章を参照。
ACE, Angiotensin converting enzyme; ACVIM, American College of Veterinary Internal Medicine; AF, atrial fibrillation; ARVC, arrhythmogenic right ventricular cardiomyopathy; ATE, arterial thromboembolism; AV, atrioventricular; BP, blood pressure; CHF, congestive heart failure; CM, cardiomyopathy; CNS, central nervous system; CO, cardiac output; CRI, constant rate infusion; DCM, dilated cardiomyopathy; dz, disease; echo, echocardiography; EP, electrophysiologic; esp., especially; GI, gastrointestinal; HCM, hypertrophic cardiomyopathy; IM, intramuscular route; IV, intravenous route; LA, left atrium; LAE, left atrial enlargement; LVOTO, left ventricular outflow tract obstruction; OHCM, obstructive HCM; PDE, phosphodiesterase; PO, orally; RAAS, renin-angiotensin-aldosterone system; RCM, restrictive cardiomyopathy; RR, respiratory rate; SA, sinoatrial; SC, subcutaneous route; SVT, supraventricular tachyarrhythmia(s).
ACE:アンジオテンシン変換酵素。ACVIM:American College of Veterinary Internal Medicine(米国内科専門医大学)。AF:心房細動。ARVC:不整脈原性右室心筋症。ATE:動脈血栓塞栓症。AV:房室。BP:血圧。CHF:うっ血性心不全。CM:心筋症。CNS:中枢神経系。CO:心拍出量。CRI:持続定速注入。DCM:拡張型心筋症。dz:疾患。echo:心エコー検査。EP:電気生理学的。esp.:特に。GI:消化管。HCM:肥大型心筋症。IM:筋肉内投与。IV:静脈内投与。LA:左心房。LAE:左心房拡大。LVOTO:左室流出路閉塞。OHCM:閉塞性肥大型心筋症。PDE:ホスホジエステラーゼ。PO:経口投与。RAAS:レニン‐アンジオテンシン‐アルドステロン系。RCM:拘束型心筋症。RR:呼吸数。SA:洞房。SC:皮下投与。SVT:上室性頻脈性不整脈。
Off-label use for cardiac applications in cats unless noted otherwise.
特記がない限り、猫の心疾患への適応外使用である。
a In case of salivation, nausea or vomiting, can be administered in an empty gelatin capsule.
a 流涎、悪心、嘔吐がみられる場合、空のゼラチンカプセルに入れて投与可能である。
b Moderate to severe LAE, low LA appendage velocities, spontaneous echo contrast, and low LA shortening fraction. Also, can be used (with caution) as cotreatment with either a factor Xa inhibitor (e.g., rivaroxaban, ch. 238) or low-dose aspirin (5 mg/cat PO q72h) in cats at very high risk of ATE.
b 中等度から重度のLAE、左心耳血流速度低下、自発性エコーコントラスト、左心房短縮率低下。さらに、ATE超高リスク猫では、Xa因子阻害薬(例:リバーロキサバン、第238章)または低用量アスピリン(5 mg/cat PO q72h)との併用治療として慎重に使用可能である。
c Extended-release formulation (not licensed for cats) is practical for use in this species. However, extended-release formulations are not designed for the feline GI tract, and instances of low plasma diltiazem concentrations, as well as intermittently very high concentrations and adverse GI and hepatic effects, have been reported.
c 徐放製剤(猫では未承認)は本種で実用的である。しかし、徐放製剤は猫の消化管向けに設計されておらず、血中ジルチアゼム濃度低下例や、断続的な著しい高濃度、および消化器・肝臓副作用が報告されている。
d Some authors describe administering cumulative daily doses of up to 10-12 mg/kg/day in certain patients with severe pulmonary edema.
d 一部著者は、重度肺水腫症例で累積1日量10-12 mg/kg/dayまで投与したと記載している。
e Taper and then stop furosemide and ACE inhibitor when substantial echocardiographic improvement is noted.
e 心エコー検査で著明な改善が認められた場合、フロセミドおよびACE阻害薬は漸減後に中止する。
MEDICAL THERAPY OF FELINE HYPERTROPHIC CARDIOMYOPATHY:猫肥大型心筋症の内科療法
ACVIM Stage B:ACVIM Stage B
Cats with subclinical HCM may live years and most (up to 80%) die from non-cardiac causes.³⁹˒⁴⁴˒⁴⁵ Thus, as in people, prophylactic therapy to prevent or delay the onset of clinical signs remains a subject of debate. Nevertheless, cats with subclinical HCM should be regularly monitored for disease progression, appearance of clinical signs, and development of CHF and ATE risk factors for those in stage B1 HCM (e.g., worsening of LAE or LVH, spontaneous echo contrast, arrhythmias etc.) using annual examinations. Cats with stage B2 HCM should be always examined in quiet conditions, with gentle restraint and minimal stress owing to the risk of acute decompensation and, if possible, owners should also monitor at home their cat’s resting or sleeping respiratory rate (normal values <30 breaths/minute; ch. 229).²⁰²
無症候性HCMの猫は何年も生存する可能性があり、その多く(最大80%)は非心疾患性原因で死亡する。³⁹˒⁴⁴˒⁴⁵ したがって、人と同様に、臨床徴候の発現を予防または遅延させるための予防的治療は依然として議論の対象となっている。それにもかかわらず、無症候性HCMの猫では、病態進行、臨床徴候の出現、ならびにStage B1 HCMにおけるCHFおよびATE危険因子(例:左房拡大[LAE]または左室肥大[LVH]の悪化、自発性エコーコントラスト、不整脈など)の発達について、年1回の検査による定期的モニタリングを行うべきである。Stage B2 HCMの猫では、急性代償不全の危険があるため、静かな環境下で、穏やかな保定と最小限のストレスで常に検査を行うべきであり、可能であればペットオーナーは自宅で安静時または睡眠時呼吸数(正常値 <30回/分;第229章)もモニタリングすべきである。²⁰²
According to the ACC/ESC Clinical Expert Consensus on human HCM, some cases at particular high risk of sudden death should receive medical treatment during the asymptomatic stage.²⁰³ The ACVIM Consensus Statement on feline cardiomyopathies similarly considers “risk categories” of cats with stage B HCM that should receive medical treatment.³ For instance, antithrombotic therapy is recommended in HCM stage B2 cats at risk for ATE (moderate to severe LAE, low LA FS%, low LA appendage velocities, and/or spontaneous echo contrast), although no PRCCT has been conducted on primary ATE prevention in cats with subclinical HCM. A PRCCT (the FATCAT study) demonstrated that clopidogrel was superior to aspirin for the prevention of recurrent cardiogenic ATE in cats.²⁰⁴ Therefore, the ACVIM Consensus Statement recommends clopidogrel as prophylactic antithrombotic treatment for cats at risk of ATE (LOE medium).³ Additionally, in cats considered at very high risk for ATE, co-treatment with clopidogrel can include aspirin (see Table 234.5) and/or an oral factor Xa inhibitor (e.g., rivaroxaban 2.5 mg q24h or 0.5-1 mg/kg/day; LOE low; ch. 238).³˒²⁰⁵⁻²⁰⁷
ヒトHCMに関するACC/ESC Clinical Expert Consensusによれば、突然死のリスクが特に高い一部症例では、無症候期から薬物治療を行うべきとされている。²⁰³ 猫心筋症に関するACVIM Consensus Statementでも同様に、薬物治療を受けるべきStage B HCM猫の「リスクカテゴリー」が考慮されている。³ 例えば、ATEリスクを有するStage B2 HCM猫(中等度〜重度のLAE、低LA FS%、低左心耳血流速度、および/または自発性エコーコントラスト)では抗血栓療法が推奨されるが、無症候性HCM猫における一次ATE予防に関する前向き無作為化対照臨床試験(PRCCT)は実施されていない。PRCCTであるFATCAT studyでは、猫の再発性心原性ATE予防においてクロピドグレルがアスピリンより優れていることが示された。²⁰⁴ そのため、ACVIM Consensus Statementでは、ATEリスクを有する猫に対する予防的抗血栓療法としてクロピドグレルを推奨している(LOE中等度)。³ さらに、ATEリスクが極めて高い猫では、クロピドグレルとの併用療法としてアスピリン(表234.5参照)および/または経口Factor Xa阻害薬(例:リバーロキサバン2.5 mg q24hまたは0.5-1 mg/kg/day;LOE低;第238章)が含まれる場合がある。³˒²⁰⁵⁻²⁰⁷
Similarly, atenolol, sotalol, or diltiazem may also be considered for treating HCM stage B cats with AF and high heart rate (LOE low, Table 234.5), and those with ventricular arrhythmias should be treated with atenolol or sotalol (LOE low, Table 234.5) (ch. 230).³ In addition to their antiarrhythmic properties, the potentially beneficial effects of beta-blockers on HCM (such as atenolol, a beta1-selective beta-blocker) are mainly attributable to their negative chronotropic and inotropic effects, with subsequent prolongation of the diastolic phase and reduced LVOTO respectively. Both can result in reduced myocardial oxygen demand (i.e., reduced myocardial ischemia).²⁰³˒²⁰⁸ Atenolol may therefore be considered for cats with stage B OHCM and severe dynamic LVOTO (LOE low),³ although there is currently no evidence that dynamic LVOTO is associated with increased cardiovascular morbidity or mortality in cats.⁹⁰ Additionally, a prospective, observational, open-label, clinical cohort study failed to demonstrate an effect of atenolol (6.25 or 12.5 mg/cat q12h) on 5-year survival in cats with stage B HCM.⁷⁰
同様に、心房細動(AF)および高心拍数を伴うStage B HCM猫では、アテノロール、ソタロール、またはジルチアゼムの使用も考慮される(LOE低、表234.5)。また、心室性不整脈を有する症例ではアテノロールまたはソタロールによる治療が推奨される(LOE低、表234.5)(第230章)。³ β遮断薬(アテノロールなどのβ1選択的β遮断薬)のHCMに対する潜在的有益作用は、その抗不整脈作用に加えて、主として陰性変時作用および陰性変力作用に起因し、その結果として拡張期延長およびLVOTO低減をもたらす。両者とも心筋酸素需要を低下させる(すなわち心筋虚血を軽減する)。²⁰³˒²⁰⁸ したがって、アテノロールはStage B閉塞性HCM(OHCM)および重度動的LVOTOを有する猫で考慮され得る(LOE低)。³ しかし現在のところ、動的LVOTOが猫における心血管罹患率または死亡率増加と関連するという証拠は存在しない。⁹⁰ さらに、前向き観察オープンラベル臨床コホート研究では、アテノロール(6.25または12.5 mg/猫 q12h)がStage B HCM猫の5年生存率に影響を与えないことが示された。⁷⁰
Similarly, a PRCCT failed to identify any clinical beneficial effect of atenolol therapy (6.25 or 12.5 mg/cat q12h) over a 6-month period in cats with subclinical HCM, although treatment with atenolol was associated with significantly lower heart rate and murmur grade.²⁰⁹ Atenolol likewise has not been shown to decrease circulating cardiac NT-proBNP or cTnI concentration,²⁰⁹ as previously shown in a pilot study involving Maine Coon cats with stage B HCM and severe LVH.²¹⁰ These results suggest a lack of beneficial effect of atenolol on myocardial ischemia and myocyte death.²¹⁰ Lastly, atenolol decreases LA function and flow velocity in the left auricle of healthy cats, two known risk factors for LAE and ATE, raising the issue of potential deleterious effects if used in feline HCM.²¹¹
同様に、PRCCTでは、無症候性HCM猫に対するアテノロール療法(6.25または12.5 mg/猫 q12h)の6か月間投与による明確な臨床的有益性は確認されなかったが、治療群では有意な心拍数低下および心雑音グレード低下が認められた。²⁰⁹ また、アテノロールは循環中NT-proBNPまたはcTnI濃度を低下させないことも示されている。²⁰⁹ これは、Stage B HCMおよび重度LVHを有するメインクーン猫を対象とした予備研究結果と一致している。²¹⁰ これらの結果は、アテノロールが心筋虚血および心筋細胞死に対して有益な効果を持たないことを示唆している。²¹⁰ 最後に、アテノロールは健常猫の左心耳における左房機能および血流速度を低下させることが示されており、これはLAEおよびATEの既知危険因子であるため、猫HCMにおいて潜在的有害作用の可能性が懸念される。²¹¹
Thus, from a practical point of view, although not specifically recommended by the ACVIM Consensus Statement, if the treatment option is chosen rather than “watchful waiting,” many clinicians now favor calcium channel blockers or antagonists of the renin-angiotensin-aldosterone system (RAAS; mainly ACE inhibitors) over atenolol in stage B feline HCM, except in cases of severe LVOTO and/or ventricular tachyarrhythmias. The rationale for using calcium channel blockers (e.g., diltiazem) includes negative chronotropic and inotropic effects, a direct positive effect on LV relaxation, coronary vasodilation, and antiarrhythmic properties.²⁰³˒²¹²˒²¹³ The rationale for prescribing RAAS antagonists is that angiotensin II and aldosterone can induce myocardial hypertrophy and fibrosis in vitro and in vivo, and in LVH animal models, both spironolactone and angiotensin II blockers may reverse such lesions and improve diastolic function, with additional vasodilatory effects for ACE inhibitors.²¹⁴⁻²¹⁹ However, no benefit on survival or onset of clinical signs has been demonstrated for either therapeutic class, and their effects on diastolic function remain unclear. A PRCCT in cats with stage B HCM revealed an increased mitral E:A ratio in the benazepril group but not the diltiazem group, without any difference between the two at the end of the study.²²⁰ Ramipril or spironolactone did not improve diastolic function in Maine Coon cats with stage B HCM assessed by a hybrid pulsed-wave TDI index in a non-myocardial location (based on Ea for some cats, summated Ea and late annular velocities for others).¹⁸⁷˒²²¹ Further studies are therefore required to accurately assess the effect of RAAS antagonists on myocardial function in occult HCM, using various non-hybrid diastolic indices from different imaging techniques (conventional Doppler combined with pulsed-wave TDI as well as 2D color TDI applied in several myocardial segments) in cats of various breeds.
したがって実臨床的観点からは、ACVIM Consensus Statementで特異的に推奨されてはいないものの、「慎重経過観察」ではなく治療を選択する場合、多くの臨床家は、重度LVOTOおよび/または心室頻拍性不整脈症例を除き、Stage B猫HCMではアテノロールよりもカルシウム拮抗薬またはレニン-アンジオテンシン-アルドステロン系(RAAS)阻害薬(主としてACE阻害薬)を選好するようになっている。カルシウム拮抗薬(例:ジルチアゼム)の理論的根拠には、陰性変時作用および陰性変力作用、左室弛緩への直接的改善作用、冠血管拡張作用、および抗不整脈作用が含まれる。²⁰³˒²¹²˒²¹³ RAAS阻害薬の理論的根拠は、アンジオテンシンIIおよびアルドステロンがin vitroおよびin vivoで心筋肥大および線維化を誘導しうる点にあり、LVH動物モデルではスピロノラクトンおよびアンジオテンシンII阻害薬の双方がこれら病変を逆転させ、拡張機能を改善する可能性が示されている。ACE阻害薬にはさらに血管拡張作用も存在する。²¹⁴⁻²¹⁹ しかし、いずれの治療群においても生存率や臨床徴候発現に対する有益性は示されておらず、拡張機能への影響も依然不明である。Stage B HCM猫を対象としたPRCCTでは、ベナゼプリル群で僧帽弁E:A比上昇が認められたが、ジルチアゼム群では認められず、試験終了時点で両群間差は存在しなかった。²²⁰ ラミプリルまたはスピロノラクトンも、メインクーン猫のStage B HCMにおいて、非心筋部位で測定されたハイブリッドパルス波TDI指標(症例によりEaまたは加算Ea+後期輪速度に基づく)では拡張機能改善を示さなかった。¹⁸⁷˒²²¹ したがって、様々な品種の猫における潜在性HCMに対するRAAS阻害薬の効果を正確に評価するためには、従来型ドプラ+パルス波TDIおよび複数心筋領域に適用した2Dカラ―TDIなど、多様な非ハイブリッド拡張機能指標を用いた追加研究が必要である。
Lastly, recent data suggest that some diets may have beneficial effects on cardiac remodeling in cats with subclinical HCM.²²² In one report, cats with stage B HCM (and particularly those without LAE) fed a diet restricted in starch and supplemented with omega-3 fatty acids showed significant decrease in end-diastolic IVS and LVFW thicknesses, with concomitant decreased circulating levels of cTnI and IGF-1.²²²
最後に、近年のデータでは、一部の食事が無症候性HCM猫の心リモデリングに有益な効果を持つ可能性が示唆されている。²²² ある報告では、Stage B HCM猫(特にLAEを伴わない症例)において、低デンプンかつω3脂肪酸補充食を給与したところ、拡張末期IVSおよびLVFW厚が有意に減少し、同時にcTnIおよびIGF-1循環濃度も低下した。²²²
ACVIM Stage C (Acute and Chronic Congestive Heart Failure; ch. 229):ACVIM Stage C(急性および慢性うっ血性心不全;第229章)
The first-line agent for controlling CHF signs is furosemide (loop diuretic).³˒²²³˒²²⁴ In acute CHF, hospital-based therapy typically includes parenteral administration of furosemide (Table 234.5), oxygen, sedation to minimize stress (e.g., butorphanol; Table 234.5), thoracocentesis in cats with severe pleural effusion (ch. 92), and cage rest (ch. 123).²²⁴ As furosemide has potential deleterious effects on renal perfusion and electrolytes, the initial emergency dosage of furosemide should be reduced as soon as signs of CHF have improved, with re-evaluation of renal parameters and electrolyte concentrations within the first week of discharge for outpatients.³˒²²⁴ Once initiated, furosemide is maintained at the lowest effective dosage every day for the rest of the cat’s life (q8-24h) or every 2 to 3 days in very rare cases of CHF related to stressful events. The goal is to maintain a resting or sleeping respiratory rate <30 breaths/minute.³˒²⁰² The degree of home monitoring and the ability (and willingness) to adjust dosages varies from owner to owner and the plan should be adapted to the owner’s capacity and wishes. Additionally, pimobendan can be considered in cats with acute signs of low cardiac output (hypotension, hypothermia, bradycardia) when dynamic LVOTO is trivial or absent, followed by constant rate infusion of dobutamine for unresponsive cases (Table 234.5).³˒²²⁴
CHF徴候制御の第一選択薬はフロセミド(ループ利尿薬)である。³˒²²³˒²²⁴ 急性CHFでは、入院下治療として通常、フロセミド注射(表234.5)、酸素投与、ストレス軽減のための鎮静(例:ブトルファノール;表234.5)、重度胸水症例に対する胸腔穿刺(第92章)、およびケージレスト(第123章)が含まれる。²²⁴ フロセミドには腎血流および電解質に対する潜在的有害作用があるため、CHF徴候改善後は速やかに初期緊急投与量を減量し、外来退院後1週間以内に腎機能パラメータおよび電解質濃度を再評価すべきである。³˒²²⁴ 一旦開始されたフロセミドは、生涯にわたり最小有効量で毎日(q8-24h)維持されるか、極めて稀なストレス関連CHF症例では2〜3日ごとに投与される。目標は安静時または睡眠時呼吸数を30回/分未満に維持することである。³˒²⁰² 在宅モニタリングの程度や投薬量調整能力(および意思)はペットオーナーにより異なるため、治療計画はオーナーの能力と希望に応じて調整すべきである。さらに、動的LVOTOが軽度または存在しない場合には、低心拍出徴候(低血圧、低体温、徐脈)を示す急性症例に対してピモベンダンを考慮でき、反応不良症例ではその後ドブタミン持続投与を行う(表234.5)。³˒²²⁴
Most often, cats with history of CHF have moderate to severe LAE, and are therefore at risk for ATE. In that case, similar prophylactic antithrombotic therapy as for ACVIM stage B HCM is recommended, with clopidogrel as first line treatment (ch. 238).³ Interestingly, a genetic polymorphism in the P2RY1 gene recently has been demonstrated to alter the response to clopidogrel therapy in HCM cats, suggesting that alternative or additional thromboprophylactic therapy should be considered in cats with the newly discovered P2RY1:A236G variant or in cats with suspected clopidogrel resistance.²²⁵
CHF既往を有する猫の多くは中等度〜重度LAEを呈しており、そのためATEリスクが高い。この場合、ACVIM Stage B HCMと同様の予防的抗血栓療法が推奨され、第一選択薬はクロピドグレルである(第238章)。³ 興味深いことに、近年P2RY1遺伝子多型がHCM猫におけるクロピドグレル反応性に影響することが示されており、新たに発見されたP2RY1:A236G変異保有猫またはクロピドグレル抵抗性が疑われる猫では、代替または追加の血栓予防療法を考慮すべき可能性が示唆されている。²²⁵
In addition to furosemide and antithrombotics, other drugs (most commonly diltiazem, ACE inhibitors, and/or pimobendan) are commonly prescribed in ACVIM stage C HCM cats, although the beneficial effects on long-term survival warrant further investigation.³˒²¹³˒²²⁶⁻²³⁷ Diltiazem therapy for cats with ACVIM stage C HCM was well tolerated and was associated with improved clinical signs and several imaging variables (e.g., isovolumic relaxation time), with 94% survival at 6-months in a non-placebo controlled prospective study.²¹³ In a non-blinded non-placebo-controlled prospective trial, the addition of benazepril to long-acting diltiazem was also well tolerated with some beneficial effects on clinical signs and LVH, but no reported survival data.²²⁷ The interim results of the Multicenter Feline Chronic Heart Failure Study for cats with CHF treated with furosemide (including 80% HCM cats), showed that the survival rate was highest in those receiving enalapril (median survival = 920 days), similar in cats treated with diltiazem (227 days) or placebo (235 days), and lowest in cats treated with atenolol (72 days).²²⁸ However, the differences between treatment groups were not statistically significant, partly due to the small number of cats in each group (personal communication, Dr. Philip R. Fox). Additionally, a PRCCT showed that long-term treatment of cats with heart disease using benazepril (for up to 2 years) was well tolerated, but no evidence of benefit was detected.²²⁹ However, cats included in this trial had various heart diseases (both congenital and acquired) of different stages, which precluded relevant conclusions from being drawn regarding ACVIM stage C HCM.²²⁹ Lastly, according to the ACVIM Consensus Statement, pimobendan (Table 234.5) can be considered in cats with ACVIM stage C HCM, provided that they do show clinically relevant LVOTO (LOE low), as its positive inotropic action could potentially lead to worsening of LVOTO with subsequent systemic hypotension, as already reported.³˒²³⁰⁻²³³ Nevertheless, several studies have shown that in most cats with OHCM, pimobendan does not significantly increase LVOTO and improved LA function could at least partially explain some of the beneficial effects reported in cats with HCM.²³⁴⁻²³⁷
フロセミドおよび抗血栓薬に加えて、他の薬剤(最も一般的にはジルチアゼム、ACE阻害薬、および/またはピモベンダン)もACVIM Stage C HCM猫で広く使用されているが、長期生存率への有益性についてはさらなる検討が必要である。³˒²¹³˒²²⁶⁻²³⁷ ACVIM Stage C HCM猫に対するジルチアゼム療法は良好に忍容され、臨床徴候および複数の画像変数(例:等容性弛緩時間)の改善と関連し、非プラセボ対照前向き試験では6か月生存率94%が報告された。²¹³ 非盲検・非プラセボ対照前向き試験では、長時間作用型ジルチアゼムへのベナゼプリル追加も良好に忍容され、臨床徴候およびLVHに一定の有益効果を示したが、生存データは報告されていない。²²⁷ フロセミド治療を受けたCHF猫(80%がHCM)を対象としたMulticenter Feline Chronic Heart Failure Study中間解析では、エナラプリル投与群の生存期間中央値が最長(920日)であり、ジルチアゼム群(227日)およびプラセボ群(235日)は類似し、アテノロール群(72日)が最短であった。²²⁸ しかし、群間差は統計学的有意差を示さなかった。これは各群症例数が少なかったことが一因と考えられた(Dr. Philip R. Fox 私信)。さらにPRCCTでは、心疾患猫に対するベナゼプリル長期投与(最大2年間)は良好に忍容されたが、有益性は確認されなかった。²²⁹ ただし、この試験には様々なステージの先天性および後天性心疾患が含まれていたため、ACVIM Stage C HCMに関する有意義な結論は導けなかった。²²⁹ 最後に、ACVIM Consensus Statementによれば、臨床的に重要なLVOTOを有するACVIM Stage C HCM猫ではピモベンダン(表234.5)を考慮できる(LOE低)。³ これはその陽性変力作用によりLVOTO悪化と続発性全身性低血圧を招く可能性が報告されているためである。³˒²³⁰⁻²³³ しかし複数研究では、大部分のOHCM猫においてピモベンダンはLVOTOを有意に増悪させず、左房機能改善がHCM猫における有益効果の少なくとも一部を説明し得ることが示されている。²³⁴⁻²³⁷
ACVIM Stage C (ATE):ACVIM Stage C(ATE)
See ch. 238.
第238章参照。
ACVIM Stage D:ACVIM Stage D
In cases of medically refractory pleural effusion, periodic thoracocentesis (pleurocentesis) is needed (ch. 92). The daily furosemide dosage should be increased in an attempt to control respiratory signs due to CHF, and in cats with persistent signs despite furosemide dosages >6 mg/kg, torsemide (another loop diuretic with a longer duration of action and a more potent diuretic effect than furosemide) may be considered at a starting dosage of 0.1-0.2 mg/kg PO q24h (LOE low; Table 234.5).³˒²²³ Dosages must be titrated carefully for each cat, and like for furosemide, the lowest effective dosage should be prescribed. Cats should be monitored regularly for hydration status, renal function, and circulating electrolyte concentrations (especially potassium, sodium, calcium, magnesium). Cats with severe CHF may require a second loop diuretic administration (i.e., furosemide) 12h after each dose of torsemide.²³⁸
内科的管理抵抗性胸水症例では、定期的胸腔穿刺(pleurocentesis)が必要となる(第92章)。CHFによる呼吸徴候制御のため、フロセミド1日投与量を増量すべきであり、6 mg/kg超のフロセミド投与にもかかわらず徴候が持続する猫では、トルセミド(フロセミドより作用持続時間が長く、利尿作用が強力な別のループ利尿薬)を0.1-0.2 mg/kg PO q24hで開始することが考慮される(LOE低;表234.5)。³˒²²³ 投与量は症例ごとに慎重に調整すべきであり、フロセミド同様、最小有効量を使用すべきである。猫では脱水状態、腎機能、および循環電解質濃度(特にカリウム、ナトリウム、カルシウム、マグネシウム)を定期的にモニタリングすべきである。重度CHF症例では、トルセミド各投与12時間後に第2のループ利尿薬(すなわちフロセミド)追加投与が必要となる場合がある。²³⁸
Owing to its positive inotropic properties, pimobendan is recommended in cats with systolic dysfunction (LOE low),³ as observed in cats with end-stage HCM (Table 234.5). Spironolactone can also be considered in cats with ACVIM stage D HCM (Table 234.5).³ In one report, ulcerative facial dermatitis was found in 4/13 cats (31%) ∼2.5 months after starting spironolactone treatment (2 mg/kg PO q12h).²³⁹ This adverse skin reaction, which was reversible after drug discontinuation, suggested that lower spironolactone dosages should be used in cats. In a subsequent study, spironolactone was well tolerated by 9 cats with CHF at a median dosage of 2.83 mg/kg (range: 2.1-3.4 mg/kg) over a 15-month period.²³⁹
その陽性変力作用により、ピモベンダンは収縮機能障害を伴う猫(LOE低)に推奨される。³ これは末期HCM猫で認められる所見である(表234.5)。スピロノラクトンもACVIM Stage D HCM猫で考慮可能である(表234.5)。³ ある報告では、スピロノラクトン治療(2 mg/kg PO q12h)開始約2.5か月後に13例中4例(31%)で潰瘍性顔面皮膚炎が認められた。²³⁹ この皮膚有害反応は薬剤中止後に可逆的であり、猫ではより低用量スピロノラクトンを使用すべき可能性が示唆された。後続研究では、CHF猫9例に対し中央値2.83 mg/kg(範囲2.1-3.4 mg/kg)のスピロノラクトンを15か月間投与したところ、良好な忍容性が確認された。²³⁹
Lastly, as in people and dogs, cardiac cachexia has been shown to be common in cats with CHF (ch. 157). The association between cachexia and reduced survival time has been demonstrated, with underweight cats having significantly shorter survival times than cats without cachexia and overweight cats.³˒¹¹⁵ Although diets with a high sodium content should be avoided in cats with refractory CHF, calorie intake should be prioritized over restriction of sodium intake.³
最後に、人および犬と同様に、心臓悪液質はCHF猫でも一般的であることが示されている(第157章)。悪液質と生存期間短縮との関連が示されており、低体重猫では悪液質のない猫や過体重猫と比較して有意に短い生存期間を示した。³˒¹¹⁵ 難治性CHF猫では高ナトリウム食を避けるべきであるが、ナトリウム制限よりもカロリー摂取維持を優先すべきである。³
OTHER PRIMARY CARDIOMYOPATHIES:その他の原発性心筋症
No PRCCT has been specifically conducted to assess treatment of cats with RCM. Management of feline RCM and HCM is therefore similar, as both diseases are pathophysiologically characterized by diastolic dysfunction with subsequent CHF.
RCM猫の治療評価を目的とした前向き無作為化対照臨床試験(PRCCT)は、これまで特異的には実施されていない。そのため、猫RCMとHCMの管理は類似している。これは両疾患が病態生理学的に拡張機能障害を特徴とし、その結果としてCHFを引き起こすためである。
In cats with DCM, positive inotropic therapy is indicated in addition to CHF and prophylactic antithrombotic therapy, whereas negative inotropic agents (e.g., diltiazem, atenolol) should be avoided. Digoxin is a weak inotrope, and therefore it is mainly prescribed for its antiarrhythmic properties in cases of supraventricular tachycardias (Table 234.5).²⁴⁰ Conversely, pimobendan is recommended in cats with DCM.³ Added to standard therapy (furosemide, taurine, ACE inhibitor, with or without digoxin), pimobendan improves survival in cats with non-taurine responsive DCM although the prognosis remains poor (median survival time = 49 days).¹¹⁴ Owing to the limitations regarding identification of cats with taurine deficiency-induced myocardial failure, some authors also recommend taurine supplementation in cats with echocardiographic DCM phenotype, regardless of blood/plasma taurine concentrations.¹⁰⁸˒¹⁰⁹˒¹¹⁴
DCM猫では、CHF治療および予防的抗血栓療法に加えて、陽性変力作用薬が適応となる。一方、陰性変力作用薬(例:ジルチアゼム、アテノロール)は避けるべきである。ジゴキシンは弱い陽性変力薬であり、そのため主として上室性頻拍症例における抗不整脈作用目的で処方される(表234.5)。²⁴⁰ 一方、ピモベンダンはDCM猫で推奨される。³ 標準治療(フロセミド、タウリン、ACE阻害薬、必要に応じてジゴキシン)に追加することで、ピモベンダンはタウリン反応性ではないDCM猫の生存期間を延長するが、予後は依然として不良である(生存期間中央値49日)。¹¹⁴ タウリン欠乏誘発性心筋不全猫の同定には限界があるため、一部の著者は、血液/血漿タウリン濃度に関係なく、心エコー検査上DCM表現型を示す猫に対してタウリン補充を推奨している。¹⁰⁸˒¹⁰⁹˒¹¹⁴
Management of feline ARVC is usually similar to that of DCM. Refractory cases of clinically overt ventricular tachycardia (e.g., syncopal and/or hypotensive tachyarrhythmia) can be treated with lidocaine IV or esmolol IV (Table 234.5). Sotalol may be prescribed for long-term oral treatment but its negative inotropic effects can be problematic (Table 234.5).¹²⁹
猫ARVCの管理は通常DCMと類似している。臨床的に明らかな難治性心室頻拍(例:失神および/または低血圧性頻拍性不整脈)症例では、リドカイン静脈内投与またはエスモロール静脈内投与による治療が可能である(表234.5)。長期経口治療としてソタロールを使用する場合もあるが、その陰性変力作用が問題となる可能性がある(表234.5)。¹²⁹
Management of feline NSCM is based on the predominant myocardial phenotype, i.e., medical treatment of predominant diastolic or systolic dysfunction being similar to that of HCM or DCM, respectively.
猫NSCMの管理は、優勢な心筋表現型に基づいて行われる。すなわち、優勢な拡張機能障害または収縮機能障害に対する内科治療は、それぞれHCMまたはDCMの治療に準じる。
REFERENCES:
1. Fox P. Feline cardiomyopathies. In: Fox P, Sisson D, Moise N, eds. Textbook of Canine and Feline Cardiology. 2nd ed. WB Saunders; 1999:621–678.
2. Kittleson M.D, Meurs K.M, Munro M.J, et al. Familial hypertrophic cardiomyopathy in Maine Coon cats: an animal model of human disease. Circulation. 1999;99:3172–3180.
3. Luis Fuentes V, Abbott J, Chetboul V, et al. ACVIM consensus statement guidelines for the classification, diagnosis, and management of cardiomyopathies in cats. J Vet Intern Med. 2020;34:1062–1077.
4. Ferasin L. Feline myocardial disease. 1: Classification, pathophysiology and clinical presentation. J Feline Med Surg. 2009;11:3–13.
5. Ferasin L. Feline myocardial disease 2: diagnosis, prognosis and clinical management. J Feline Med Surg. 2009;11:183–194.
6. Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br Heart J. 1980;44:672–673.
7. Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the definition and classification of cardiomyopathies. Circulation. 1996;93:841–842.
8. Maron B.J, Towbin J.A, Thiene G, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816.
9. Thiene G, Corrado D, Basso C. Cardiomyopathies: is it time for a molecular classification? Eur Heart J. 2004;25:1772–1775.
10. Thiene G, Corrado D, Basso C. Revisiting definition and classification of cardiomyopathies in the era of molecular medicine. Eur Heart J. 2008;29:144–146.
11. Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276.
12. Arbustini E, Narula N, Dec G.W, et al. The MOGE(S) classification for a phenotype-genotype nomenclature of cardiomyopathy: endorsed by the World Heart Federation. J Am Coll Cardiol. 2013;62:2046–2072.
13. Rapezzi C, Arbustini E, Caforio A.L, et al. Diagnostic work-up in cardiomyopathies: bridging the gap between clinical phenotypes and final diagnosis. A position statement from the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34:1448–1458.
14. Sisakian H. Cardiomyopathies: evolution of pathogenesis concepts and potential for new therapies. World J Cardiol. 2014;6:478–494.
15. Fox P.R, Maron B.J, Basso C, et al. Spontaneously occurring arrhythmogenic right ventricular cardiomyopathy in the domestic cat: A new animal model similar to the human disease. Circulation. 2000;102:1863–1870.
16. Fox P.R. Endomyocardial fibrosis and restrictive cardiomyopathy: pathologic and clinical features. J Vet Cardiol. 2004;6:25–31.
17. Fox P.R, Basso C, Thiene G, et al. Spontaneously occurring restrictive nonhypertrophied cardiomyopathy in domestic cats: a new animal model of human disease. Cardiovasc Pathol. 2014;23:28–34.
18. Galderisi M. The new European definition of cardiomyopathies: which space for muscle dystrophies? Eur Heart J. 2008;29:1591–1592.
19. Elliott P.M. Classification of cardiomyopathies: evolution or revolution? J Am Coll Cardiol. 2013;62:2073–2074.
20. Riesen S.C, Kovacevic A, Lombard C.W, et al. Prevalence of heart disease in symptomatic cats: an overview from 1998 to 2005. Schweiz Arch Tierheilkd. 2007;149:65–71.
21. Spalla I, Locatelli C, Riscazzi G, et al. Survival in cats with primary and secondary cardiomyopathies. J Feline Med Surg. 2016;18:501–509.
22. Ferasin L, Sturgess C.P, Cannon M.J, et al. Feline idiopathic cardiomyopathy: a retrospective study of 106 cats (1994-2001). J Feline Med Surg. 2003;5:151–159.
23. Silbiger J.J. Left ventricular false tendons: anatomic, echocardiographic, and pathophysiologic insights. J Am Soc Echocardiogr. 2013;26:582–588.
24. Philip S, Cherian K.M, Wu M.H, et al. Left ventricular false tendons: echocardiographic, morphologic, and histopathologic studies and review of the literature. Pediatr Neonatol. 2011;52:279–286.
25. Gerlis L.M, Wright H.M, Wilson N, et al. Left ventricular bands. A normal anatomical feature. Br Heart J. 1984;52:641–647.
26. Fox P. Cardiovascular pathology. In: Fox P, Sisson D, Moise N, eds. Textbook of Canine and Feline Cardiology. 2nd ed. WB Saunders; 1999:817–844.
27. Liu S, Fox P.R, Tilley L.P. Excessive moderator bands in the left ventricle of 21 cats. J Am Vet Med Assoc. 1982;180:1215–1219.
28. Wolf O.A, Imgrund M, Wess G. Echocardiographic assessment of feline false tendons and their relationship with focal thickening of the left ventricle. J Vet Cardiol. 2017;19:14–23.
29. Schober K, Todd A. Echocardiographic assessment of left ventricular geometry and the mitral valve apparatus in cats with hypertrophic cardiomyopathy. J Vet Cardiol. 2010;12:1–16.
30. Boon J.A. Myocardial diseases. In: Boon J.A, ed. Manual of Veterinary Echocardiography. 2nd ed. Wiley-Blackwell; 2011:359–410.
31. Kittleson M.D, Fox P.R, Basso C, et al. Naturally occurring biventricular noncompaction in an adult domestic cat. J Vet Intern Med. 2017;31:527–531.
32. Gelberg H.B. Purkinje fiber dysplasia (histiocytoid cardiomyopathy) with ventricular noncompaction in a savannah kitten. Vet Pathol. 2009;46:693–697.
33. Fox P.R. Hypertrophic cardiomyopathy. Clinical and pathologic correlates. J Vet Cardiol. 2003;5:39–45.
34. Liu S.K, Maron B.J, Tilley L.P. Feline hypertrophic cardiomyopathy: gross anatomic and quantitative histologic features. Am J Pathol. 1981;102:388–395.
35. Maron B.J. Hypertrophic cardiomyopathy. In: Bonow R.O, Mann D.L, Zipes D.P, et al., eds. Braunwald’s Heart Disease. A Textbook of Cardiovascular Medicine. 9th ed. Elsevier Saunders; 2012:1582–1594.
36. Fox P.R, Liu S.K, Maron B.J. Echocardiographic assessment of spontaneously occurring feline hypertrophic cardiomyopathy. An animal model of human disease. Circulation. 1995;92:2645–2651.
37. MacLea H.B, Boon J.A, Bright J.M. Doppler echocardiographic evaluation of midventricular obstruction in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2013;27:1416–1420.
38. Peterson E.N, Moise N.S, Brown C.A, et al. Heterogeneity of hypertrophy in feline hypertrophic heart disease. J Vet Intern Med. 1993;7:183–189.
39. Trehiou-Sechi E, Tissier R, Gouni V, et al. Comparative echocardiographic and clinical features of hypertrophic cardiomyopathy in 5 breeds of cats: a retrospective analysis of 344 cases (2001-2011). J Vet Intern Med. 2012;26:532–541.
40. Visser L.C, Sloan C.Q, Stern J.A. Echocardiographic assessment of right ventricular size and function in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2017;31:668–677.
41. Carlos Sampedrano C, Chetboul V, Gouni V, et al. Systolic and diastolic myocardial dysfunction in cats with hypertrophic cardiomyopathy or systemic hypertension. J Vet Intern Med. 2006;20:1106–1115.
42. Carlos Sampedrano C, Chetboul V, Mary J, et al. Prospective echocardiographic and tissue Doppler imaging screening of a population of Maine Coon cats tested for the A31P mutation in the myosin-binding protein C gene: a specific analysis of the heterozygous status. J Vet Intern Med. 2009;23:91–99.
43. Khor K.H, Campbell F.E, Owen H, et al. Myocardial collagen deposition and inflammatory cell infiltration in cats with pre-clinical hypertrophic cardiomyopathy. Vet J. 2015;203:161–168.
44. Rush J.E, Freeman L.M, Fenollosa N.K, et al. Population and survival characteristics of cats with hypertrophic cardiomyopathy: 260 cases (1990-1999). J Am Vet Med Assoc. 2002;220:202–207.
45. Payne J, Luis Fuentes V, Boswood A, et al. Population characteristics and survival in 127 referred cats with hypertrophic cardiomyopathy (1997 to 2005). J Small Anim Pract. 2010;51:540–547.
46. Granström S, Godiksen M.T, Christiansen M, et al. Prevalence of hypertrophic cardiomyopathy in a cohort of British Shorthair cats in Denmark. J Vet Intern Med. 2011;25:866–871.
47. Payne J.R, Brodbelt D.C, Luis Fuentes V. Cardiomyopathy prevalence in 780 apparently healthy cats in rehoming centres (the CatScan study). J Vet Cardiol. 2015;17(Suppl 1):S244–257.
48. Mazzarotto F, Olivotto I, Boschi B, et al. Contemporary insights into the genetics of hypertrophic cardiomyopathy: toward a new era in clinical testing? J Am Heart Assoc. 2020;9:e015473.
49. Wijnker P.J.M, van der Velden J. Mutation-specific pathology and treatment of hypertrophic cardiomyopathy in patients, mouse models and human engineered heart tissue. Biochim Biophys Acta Mol Basis Dis. 2020;1866:165774.
50. Geisterfer-Lowrance A.A, Kass S, Tanigawa G, et al. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999–1006.
51. Meurs K.M, Sanchez X, David R.M, et al. A cardiac myosin binding protein C mutation in the Maine Coon cat with familial hypertrophic cardiomyopathy. Hum Mol Genet. 2005;14:3587–3593.
52. Fries R, Heaney A.M, Meurs K.M. Prevalence of the myosin-binding protein C mutation in Maine Coon cats. J Vet Intern Med. 2008;22:893–896.
53. Mary J, Chetboul V, Carlos Sampedrano C, et al. Prevalence of the MYBPC3-A31P mutation in a large European feline population and association with hypertrophic cardiomyopathy in the Maine Coon breed. J Vet Cardiol. 2010;12:155–161.
54. Longeri M, Ferrari P, Knafelz P, et al. Myosin-binding protein C DNA variants in domestic cats (A31P, A74T, R820W) and their association with hypertrophic cardiomyopathy. J Vet Intern Med. 2013;27:275–285.
55. Wess G, Schinner C, Weber K, et al. Association of A31P and A74T polymorphisms in the myosin binding protein C3 gene and hypertrophic cardiomyopathy in Maine Coon and other breed cats. J Vet Intern Med. 2010;24:527–532.
56. McNamara J.W, Schuckman M, Becker R.C, et al. A novel homozygous intronic variant in TNNT2 associates with feline cardiomyopathy. Front Physiol. 2020;11:608473.
57. Meurs K.M, Norgard M.M, Ederer M.M, et al. A substitution mutation in the myosin binding protein C gene in Ragdoll hypertrophic cardiomyopathy. Genomics. 2007;90:261–264.
58. Borgeat K, Casamian-Sorrosal D, Helps C, et al. Association of the myosin binding protein C3 mutation (MYBPC3 R820W) with cardiac death in a survey of 236 Ragdoll cats. J Vet Cardiol. 2014;16:73–80.
59. Silverman S.J, Stern J.A, Meurs K.M. Hypertrophic cardiomyopathy in the Sphynx cat: a retrospective evaluation of clinical presentation and heritable etiology. J Feline Med Surg. 2012;14:246–249.
60. Chetboul V, Petit A, Gouni V, et al. Prospective echocardiographic and tissue Doppler screening of a large Sphynx cat population: reference ranges, heart disease prevalence and genetic aspects. J Vet Cardiol. 2012;14:497–509.
61. März I, Wilkie L.J, Harrington N, et al. Familial cardiomyopathy in Norwegian Forest cats. J Feline Med Surg. 2015;17:681–691.
62. Nakagawa K, Takemura N, Machida N, et al. Hypertrophic cardiomyopathy in a mixed breed cat family. J Vet Med Sci. 2002;64:619–621.
63. Kraus M.S, Calvert C.A, Jacobs G.J. Hypertrophic cardiomyopathy in a litter of five mixed-breed cats. J Am Anim Hosp Assoc. 1999;35:293–296.
64. Meurs K.M, Williams B.G, DeProspero D, et al. A deleterious mutation in the ALMS1 gene in a naturally occurring model of hypertrophic cardiomyopathy in the Sphynx cat. Orphanet J Rare Dis. 2021;16:108.
65. Schipper T, Van Poucke M, Sonck L, et al. A feline orthologue of the human MYH7 c.5647G>A (p.(Glu1883Lys)) variant causes hypertrophic cardiomyopathy in a domestic shorthair cat. Eur J Hum Genet. 2019;27:1724–1730.
66. O’Donnell K, Adin D, Atkins C.E, et al. Absence of known feline MYH7 and MYBPC3 variants in a diverse cohort of cats with hypertrophic cardiomyopathy. Anim Genet. 2021;52:542–544.
67. Golden A.L, Bright J.M. Use of relaxation half-time as an index of ventricular relaxation in clinically normal cats and cats with hypertrophic cardiomyopathy. Am J Vet Res. 1990;51:1352–1356.
68. Payne J.R, Borgeat K, Connolly D.J, et al. Prognostic indicators in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2013;27:1427–1436.
69. Riesen S.C, Schober K.E, Smith D.N, et al. Effects of ivabradine on heart rate and left ventricular function in healthy cats and cats with hypertrophic cardiomyopathy. Am J Vet Res. 2012;73:202–212.
70. Schober K.E, Zientek J, Li X, et al. Effect of treatment with atenolol on 5-year survival in cats with preclinical (asymptomatic) hypertrophic cardiomyopathy. J Vet Cardiol. 2013;15:93–104.
71. Koffas H, Dukes-McEwan J, Corcoran B.M, et al. Pulsed tissue Doppler imaging in normal cats and cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2006;20:65–77.
72. MacDonald K.A, Kittleson M.D, Kass P.H, et al. Tissue Doppler imaging in Maine Coon cats with a mutation of myosin binding protein C with or without hypertrophy. J Vet Intern Med. 2007;21:232–237.
73. Chetboul V, Carlos Sampedrano C, Gouni V, et al. Two-dimensional color tissue Doppler imaging detects myocardial dysfunction before occurrence of hypertrophy in a young Maine Coon cat. Vet Radiol Ultrasound. 2006;47:295–300.
74. Schober K.E, Chetboul V. Echocardiographic evaluation of left ventricular diastolic function in cats: hemodynamic determinants and pattern recognition. J Vet Cardiol. 2015;17(Suppl 1):S102–S133.
75. Côté E, MacDonald K.A, Meurs K.M, et al. Congestive heart failure. In: Côté E, MacDonald K.A, Meurs K.M, et al., eds. Feline Cardiology. Wiley-Blackwell; 2011:257–302.
76. Schober K.E, Maerz I. Assessment of left atrial appendage flow velocity and its relation to spontaneous echocardiographic contrast in 89 cats with myocardial disease. J Vet Intern Med. 2006;20:120–130.
77. Laste N.J, Harpster N.K. A retrospective study of 100 cases of feline distal aortic thromboembolism: 1977-1993. J Am Anim Hosp Assoc. 1995;31:492–500.
78. Bédard C, Lanevschi-Pietersma A, Dunn M. Evaluation of coagulation markers in the plasma of healthy cats and cats with asymptomatic hypertrophic cardiomyopathy. Vet Clin Pathol. 2007;36:167–172.
79. Stokol T, Brooks M, Rush J.E, et al. Hypercoagulability in cats with cardiomyopathy. J Vet Intern Med. 2008;22:546–552.
80. Koffas H, Dukes-McEwan J, Corcoran B.M, et al. Colour M-mode tissue Doppler imaging in healthy cats and cats with hypertrophic cardiomyopathy. J Small Anim Pract. 2008;49:330–338.
81. Sherrid M.V, Gunsburg D.Z, Moldenhauer S, et al. Systolic anterior motion begins at low left ventricular outflow tract velocity in obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2000;36:1344–1354.
82. Atkins C.E, Gallo A.M, Kurzman I.D, et al. Risk factors, clinical signs, and survival in cats with a clinical diagnosis of idiopathic hypertrophic cardiomyopathy: 74 cases (1985-1989). J Am Vet Med Assoc. 1992;201:613–618.
83. Wilkie L.J, Smith K, Luis F.V. Cardiac pathology findings in 252 cats presented for necropsy; a comparison of cats with unexpected death versus other deaths. J Vet Cardiol. 2015;17:S329–S340.
84. Schober K.E, Maerz I, Ludewig E, et al. Diagnostic accuracy of electrocardiography and thoracic radiography in the assessment of left atrial size in cats: comparison with transthoracic 2-dimensional echocardiography. J Vet Intern Med. 2007;21:709–718.
85. Jackson B.L, Lehmkuhl L.B, Adin D.B. Heart rate and arrhythmia frequency of normal cats compared to cats with asymptomatic hypertrophic cardiomyopathy. J Vet Cardiol. 2014;16:215–225.
86. Côté E, Jaeger R. Ventricular tachyarrhythmias in 106 cats: associated structural cardiac disorders. J Vet Intern Med. 2008;22:1444–1446.
87. Bartoszuk U, Keene B.W, Baron Toaldo M, et al. Holter monitoring demonstrates that ventricular arrhythmias are common in cats with decompensated and compensated hypertrophic cardiomyopathy. Vet J. 2019;243:21–25.
88. Chetboul V, Carlos Sampedrano C, Tissier R, et al. Quantitative assessment of velocities of the annulus of the left atrioventricular valve and left ventricular free wall in healthy cats by use of two-dimensional color tissue Doppler imaging. Am J Vet Res. 2006;67:250–258.
89. Linney C.J, Dukes-McEwan J, Stephenson H.M, et al. Left atrial size, atrial function and left ventricular diastolic function in cats with hypertrophic cardiomyopathy. J Small Anim Pract. 2014;55:198–206.
90. Fox P.R, Keene B.W, Lamb K, et al. International collaborative study to assess cardiovascular risk and evaluate long-term health in cats with preclinical hypertrophic cardiomyopathy and apparently healthy cats: The REVEAL Study. J Vet Intern Med. 2018;32:930–943.
91. Kushwaha S.S, Fallon J.T, Fuster V. Restrictive cardiomyopathy. N Engl J Med. 1997;336:267–276.
92. Hare J.M. The dilated, restrictive, and infiltrative cardiomyopathies. In: Bonow R.O, Mann D.L, Zipes D.P, et al., eds. Braunwald’s Heart Disease. A Textbook of Cardiovascular Medicine. 9th ed. Elsevier Saunders; 2012:1561–1581.
93. Sisakian H. Cardiomyopathies: Evolution of pathogenesis concepts and potential for new therapies. World J Cardiol. 2014;6:478–494.
94. Falk R.H, Hershberger R.E. The dilated, restrictive, and infiltrative cardiomyopathies. In: Mann D.L, Zipes D.P, Libby P, et al., eds. Braunwald’s Heart Disease. A Textbook of Cardiovascular Medicine. 10th ed. Elsevier Saunders; 2015:1551–1573.
95. Seth S, Thatai D, Sharma S, et al. Clinico-pathological evaluation of restrictive cardiomyopathy (endomyocardial fibrosis and idiopathic restrictive cardiomyopathy) in India. Eur J Heart Fail. 2004;6:723–729.
96. Mocumbi A.O, Stothard J.R, Correia-de-Sá P, et al. Endomyocardial fibrosis: an update after 70 years. Curr Cardiol Rep. 2019;21:148.
97. Towbin J.A. Inherited cardiomyopathies. Circ J. 2014;78:2347–2356.
98. Parvatiyar M.S, Pinto J.R, Dweck D, et al. Cardiac troponin mutations and restrictive cardiomyopathy. J Biomed Biotechnol. 2010;2010:350706.
99. Muchtar E, Blauwet L.A, Gertz M.A. Restrictive cardiomyopathy: genetics, pathogenesis, clinical manifestations, diagnosis, and therapy. Circ Res. 2017;121:819–837.
100. Stalis I.H, Bossbaly M.J, Van Winkle T.J. Feline endomyocarditis and left ventricular endocardial fibrosis. Vet Pathol. 1995;32:122–126.
101. Chetboul V, Passavin P, Trehiou-Sechi E, et al. Clinical, epidemiological and echocardiographic features and prognostic factors in cats with restrictive cardiomyopathy: a retrospective study of 92 cases (2001-2015). J Vet Intern Med. 2019;33:1222–1231.
102. Kimura Y, Karakama S, Hirakawa A, et al. Pathological features and pathogenesis of the endomyocardial form of restrictive cardiomyopathy in cats. J Comp Pathol. 2016;155:190–198.
103. Kimura Y, Fukushima R, Hirakawa A, et al. Epidemiological and clinical features of the endomyocardial form of restrictive cardiomyopathy in cats: a review of 41 cases. J Vet Med Sci. 2016;78:781–784.
104. Locatelli C, Pradelli D, Campo G, et al. Survival and prognostic factors in cats with restrictive cardiomyopathy: a review of 90 cases. J Feline Med Surg. 2018;20:1138–1143.
105. Meurs K.M, Fox P.R, Magnon A.L, et al. Molecular screening by polymerase chain reaction detects panleukopenia virus DNA in formalin-fixed hearts from cats with idiopathic cardiomyopathy and myocarditis. Cardiovasc Pathol. 2000;9:119–126.
106. Donovan T.A, Balakrishnan N, Carvalho Barbosa I, et al. Bartonella spp. as a possible cause or cofactor of feline endomyocarditis-left ventricular endocardial fibrosis complex. J Comp Pathol. 2018;162:29–42.
107. Rivenes S.M, Kearney D.L, Smith E.O, et al. Sudden death and cardiovascular collapse in children with restrictive cardiomyopathy. Circulation. 2000;102:876–882.
108. Pion P.D, Kittleson M.D, Rogers Q.R, et al. Myocardial failure in cats associated with low plasma taurine: a reversible cardiomyopathy. Science. 1987;237:764–768.
109. Pion P.D. Traditional and nontraditional effective and noneffective therapies for cardiac disease in dogs and cats. Vet Clin North Am Small Anim Pract. 2004;34:187–216.
110. Schober K.E, Kent A.M, Aeffner F. Tachycardia-induced cardiomyopathy in a cat. Schweiz Arch Tierheilkd. 2014;156:133–139.
111. Meurs K.M, Stern J.A, Adin D, et al. Assessment of PDK4 and TTN gene variants in 48 Doberman Pinschers with dilated cardiomyopathy. J Am Vet Med Assoc. 2020;257:1041–1044.
112. Lawler D.F, Templeton A.J, Monti K.L. Evidence for genetic involvement in feline dilated cardiomyopathy. J Vet Intern Med. 1993;7:383–387.
113. Wess G, Domenech O, Dukes-McEwan J, et al. European Society of Veterinary Cardiology screening guidelines for dilated cardiomyopathy in Doberman Pinschers. J Vet Cardiol. 2017;19:405–415.
114. Hambrook L.E, Bennett P.F. Effect of pimobendan on the clinical outcome and survival of cats with non-taurine responsive dilated cardiomyopathy. J Feline Med Surg. 2012;14:233–239.
115. Santiago S.L, Freeman L.M, Rush J.E. Cardiac cachexia in cats with congestive heart failure: prevalence and clinical, laboratory, and survival findings. J Vet Intern Med. 2020;34:35–44.
116. Calkins H. Arrhythmogenic right ventricular dysplasia/cardiomyopathy—three decades of progress. Circ J. 2015;79:901–913.
117. Marcus F.I, McKenna W.J, Sherrill D, et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation. 2010;121:1533–1541.
118. Saguner A.M, Brunckhorst C, Duru F. Arrhythmogenic ventricular cardiomyopathy: a paradigm shift from right to biventricular disease. World J Cardiol. 2014;6:154–174.
119. Gomes J, Finlay M, Ahmed A.K, et al. Electrophysiological abnormalities precede overt structural changes in arrhythmogenic right ventricular cardiomyopathy due to mutations in desmoplakin—a combined murine and human study. Eur Heart J. 2012;33:1942–1953.
120. Basso C, Thiene G, Corrado D, et al. Arrhythmogenic right ventricular cardiomyopathy: dysplasia, dystrophy or myocarditis? Circulation. 1996;94:983–991.
121. Basso C, Fox P.R, Meurs K.M, et al. Arrhythmogenic right ventricular cardiomyopathy causing sudden cardiac death in boxer dogs: a new animal model of human disease. Circulation. 2004;109:1180–1185.
122. Santilli R.A, Bontempi L.V, Perego M. Ventricular tachycardia in English bulldogs with localised right ventricular outflow tract enlargement. J Small Anim Pract. 2011;52:574–580.
123. Caro-Vadillo A, García-Guasch L, Carretón E, et al. Arrhythmogenic right ventricular cardiomyopathy in boxer dogs: a retrospective study of survival. Vet Rec. 2013;172:268.
124. Meurs K.M, Mauceli E, Lahmers S, et al. Genome-wide association identifies a deletion in the 3’ untranslated region of striatin in a canine model of arrhythmogenic right ventricular cardiomyopathy. Hum Genet. 2010;128:315–324.
125. Meurs K.M, Stern J.A, Reina-Doreste Y, et al. Natural history of arrhythmogenic right ventricular cardiomyopathy in the boxer dog: a prospective study. J Vet Intern Med. 2014;28:1214–1220.
126. Oyama M.A, Reiken S, Lehnart S.E, et al. Arrhythmogenic right ventricular cardiomyopathy in Boxer dogs is associated with calstabin2 deficiency. J Vet Cardiol. 2008;10:1–10.
127. Oxford E.M, Danko C.G, Kornreich B.G, et al. Ultrastructural changes in cardiac myocytes from Boxer dogs with arrhythmogenic right ventricular cardiomyopathy. J Vet Cardiol. 2011;13:101–113.
128. Oxford E.M, Everitt M, Coombs W, et al. Molecular composition of the intercalated disc in a spontaneous canine animal model of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Heart Rhythm. 2007;4:1196–1205.
129. Fox P.R. Arrhythmogenic right ventricular cardiomyopathy in cats. Web.chapter 58. In: Bonagura J.D, Twedt D.C, eds. Kirk’s Current Veterinary Therapy XV. Elsevier; 2014:e277.
130. Harvey A.M, Battersby I.A, Faena M, et al. Arrhythmogenic right ventricular cardiomyopathy in two cats. J Small Anim Pract. 2005;46:151–156.
131. Ciaramella P, Basso C, Di Loria A, et al. Arrhythmogenic right ventricular cardiomyopathy associated with severe left ventricular involvement in a cat. J Vet Cardiol. 2009;11:41–45.
132. Paige C.F, Abbott J.A, Elvinger F, et al. Prevalence of cardiomyopathy in apparently healthy cats. J Am Vet Med Assoc. 2009;234:1398–1403.
133. Floria M, Tinica G, Grecu M. Left ventricular non-compaction—challenges and controversies. Maedica (Buchar). 2014;9:282–288.
134. Cannon 3rd. R.O, Rosing D.R, Maron B.J, et al. Myocardial ischemia in patients with hypertrophic cardiomyopathy: contribution of inadequate vasodilator reserve and elevated left ventricular filling pressures. Circulation. 1985;71:234–243.
135. Spirito P, Maron B.J, Bonow R.O, et al. Occurrence and significance of progressive left ventricular wall thinning and relative cavity dilatation in hypertrophic cardiomyopathy. Am J Cardiol. 1987;60:123–129.
136. Kawashima T, Yokota Y, Yokoyama M, et al. Pathological analysis of hypertrophic cardiomyopathy simulating dilated cardiomyopathy. Acta Pathol Jpn. 1993;43:304–312.
137. Cesta M.F, Baty C.J, Keene B.W, et al. Pathology of end-stage remodeling in a family of cats with hypertrophic cardiomyopathy. Vet Pathol. 2005;42:458–467.
138. Baty C.J, Malarkey D.E, Atkins C.E, et al. Natural history of hypertrophic cardiomyopathy and aortic thromboembolism in a family of domestic shorthair cats. J Vet Intern Med. 2001;15:595–599.
139. Ino T, Nishimoto K, Okubo M, et al. Apoptosis as a possible cause of wall thinning in end-stage hypertrophic cardiomyopathy. Am J Cardiol. 1997;79:1137–1141.
140. Fujino N, Shimizu M, Ino H, et al. A novel mutation Lys273Glu in the cardiac troponin T gene shows high degree of penetrance and transition from hypertrophic to dilated cardiomyopathy. Am J Cardiol. 2002;89:29–33.
141. Liu S.K, Peterson M.E, Fox P.R. Hypertrophic cardiomyopathy and hyperthyroidism in the cat. J Am Vet Med Assoc. 1984;185:52–57.
142. Moise N.S, Dietze A.E, Mezza L.E, et al. Echocardiography, electrocardiography, and radiography of cats with dilatation cardiomyopathy, hypertrophic cardiomyopathy, and hyperthyroidism. Am J Vet Res. 1986;47:1476–1486.
143. Connolly D.J, Guitian J, Boswood A, et al. Serum troponin I levels in hyperthyroid cats before and after treatment with radioactive iodine. J Feline Med Surg. 2005;7:289–300.
144. Weichselbaum R.C, Feeney D.A, Jessen C.R. Relationship between selected echocardiographic variables before and after radioiodine treatment in 91 hyperthyroid cats. Vet Radiol Ultrasound. 2005;46:506–513.
145. Snyder P.S, Sadek D, Jones G.L. Effect of amlodipine on echocardiographic variables in cats with systemic hypertension. J Vet Intern Med. 2001;15:52–56.
146. Nelson L, Reidesel E, Ware W.A, et al. Echocardiographic and radiographic changes associated with systemic hypertension in cats. J Vet Intern Med. 2002;16:418–425.
147. Chetboul V, Lefebvre H.P, Pinhas C, et al. Spontaneous feline hypertension: clinical and echocardiographic abnormalities, and survival rate. J Vet Intern Med. 2003;17:89–95.
148. Henik R.A, Stepien R.L, Bortnowski H.B. Spectrum of M-mode echocardiographic abnormalities in 75 cats with systemic hypertension. J Am Anim Hosp Assoc. 2004;40:359–363.
149. Campbell F.E, Kittleson M.D. The effect of hydration status on the echocardiographic measurements of normal cats. J Vet Intern Med. 2007;21:1008–1015.
150. Carter T.D, Pariaut R, Snook E, et al. Multicentric lymphoma mimicking decompensated hypertrophic cardiomyopathy in a cat. J Vet Intern Med. 2008;22:1345–1347.
151. Rolim V.M, Casagrande R.A, Wouters A.T, et al. Myocarditis caused by feline immunodeficiency virus in five cats with hypertrophic cardiomyopathy. J Comp Pathol. 2016;154:3–8.
152. Simpson K.E, Devine B.C, Gunn-Moore D. Suspected toxoplasma-associated myocarditis in a cat. J Feline Med Surg. 200;7:203–208.
153. Joseph J.L, Oxford E.M, Santilli R.A. Transient myocardial thickening in a Bartonella henselae-positive cat. J Vet Cardiol. 2018;20:198–203.
154. Gaschen L, Lang J, Lin S, et al. Cardiomyopathy in dystrophin-deficient hypertrophic feline muscular dystrophy. J Vet Intern Med. 1999;13:346–356.
155. Chetboul V, Blot S, Carlos Sampedrano C, et al. Tissue Doppler imaging for detection of radial and longitudinal myocardial dysfunction in a family of cats affected by dystrophin-deficient hypertrophic muscular dystrophy. J Vet Intern Med. 2006;20:640–647.
156. Ployngam T, Tobias A.H, Smith S.A, et al. Hemodynamic effects of methylprednisolone acetate administration in cats. Am J Vet Res. 2006;67:583–587.
157. Peterson M.E, Taylor R.S, Greco D.S, et al. Acromegaly in 14 cats. J Vet Intern Med. 1990;4:192–201.
158. Myers J.A, Lunn K.F, Bright J.M. Echocardiographic findings in 11 cats with acromegaly. J Vet Intern Med. 2014;28:1235–1238.
159. Steele M.M, Borgeat K, Payne J.R, et al. Increased insulin-like growth factor 1 concentrations in a retrospective population of non-diabetic cats diagnosed with hypertrophic cardiomyopathy. J Feline Med Surg. 2021;23:952–958.
160. Borgeat K, Niessen S.J.M, Wilkie L, et al. Time spent with cats is never wasted: lessons learned from feline acromegalic cardiomyopathy, a naturally occurring animal model of the human disease. PLoS One. 2018;13:e0194342.
161. Novo Matos J, Pereira N, Glaus T, et al. Transient myocardial thickening in cats associated with heart failure. J Vet Intern Med. 2018;32:48–56.
162. Smith S, Dukes-McEwan J. Clinical signs and left atrial size in cats with cardiovascular disease in general practice. J Small Anim Pract. 2012;53:27–33.
163. Le Boedec K, Arnaud C, Chetboul V, et al. Relationship between paradoxical breathing and pleural diseases in dyspneic dogs and cats: 389 cases (2001-2009). J Am Vet Med Assoc. 2012;24:1095–1099.
164. Dickson D, Little C.J.L, Harris J, Rishniw M. Rapid assessment with physical examination in dyspnoeic cats: the RAPID CAT study. J Small Anim Pract. 2018;59:75–84.
165. Côté E, MacDonald K.A, Meurs K.M, et al. Radiology. In: Côté E, MacDonald K.A, Meurs K.M, et al., eds. Feline Cardiology. Wiley Blackwell; 2011:85–100.
166. Rishniw M. Radiography of feline cardiac disease. Vet Clin North Am Small Anim Pract. 2000;30:395–425.
167. Guglielmini C, Baron Toaldo M, Poser H, et al. Diagnostic accuracy of the vertebral heart score and other radiographic indices in the detection of cardiac enlargement in cats with different cardiac disorders. J Feline Med Surg. 2014;16:812–825.
168. Lister A.L, Buchanan J.W. Vertebral scale system to measure heart size in radiographs of cats. J Am Vet Med Assoc. 2000;216:210–214.
169. Ghadiri A, Avizeh R, Rasekh A, et al. Radiographic measurement of vertebral heart size in healthy stray cats. J Feline Med Surg. 2008;10:61–65.
170. Sleeper M.M, Roland R, Drobatz K.J. Use of the vertebral heart scale for differentiation of cardiac and noncardiac causes of respiratory distress in cats: 67 cases (2002-2003). J Am Vet Med Assoc. 2013;242:366–371.
171. Winter M.D, Giglio R.F, Berry C.R, et al. Associations between “valentine” heart shape, atrial enlargement and cardiomyopathy in cats. J Feline Med Surg. 2015;17:447–452.
172. Oura T.J, Young A.N, Keene B.W, et al. A valentine-shaped cardiac silhouette in feline thoracic radiographs is primarily due to left atrial enlargement. Vet Radiol Ultrasound. 2015;56:245–250.
173. Benigni L, Morgan N, Lamb C.R. Radiographic appearance of cardiogenic pulmonary oedema in 23 cats. J Small Anim Pract. 2009;50:9–14.
174. Ward J.L, Lisciandro G.R, Ware W.A, et al. Evaluation of point-of-care thoracic ultrasound and NT-proBNP for the diagnosis of congestive heart failure in cats with respiratory distress. J Vet Intern Med. 2018;32:1530–1540.
175. Ward JL, Lisciandro G.R, Keene B.W, et al. Accuracy of point-of-care lung ultrasonography for the diagnosis of cardiogenic pulmonary edema in dogs and cats with acute dyspnea. J Am Vet Med Assoc. 2017;250:666–675.
176. Loughran K.A, Rush J.E, Rozanski E.A, et al. The use of focused cardiac ultrasound to screen for occult heart disease in asymptomatic cats. J Vet Intern Med. 2019;33:1892–1901.
177. Chetboul V, Concordet D, Pouchelon J.L, et al. Effects of inter- and intra-observer variability on echocardiographic measurements in awake cats. J Vet Med A Physiol Pathol Clin Med. 2003;50:326–331.
178. Häggström J, Andersson Å.O, Falk T, et al. Effect of body weight on echocardiographic measurements in 19,866 pure-bred cats with or without heart disease. J Vet Intern Med. 2016;30:1601–1611.
179. Abbott J.A, MacLean H.N. Two-dimensional echocardiographic assessment of the feline left atrium. J Vet Intern Med. 2006;20:111–119.
180. Duler L, Scollan K.F, LeBlanc N.L. Left atrial size and volume in cats with primary cardiomyopathy with and without congestive heart failure. J Vet Cardiol. 2019;24:36–47.
181. Chetboul V. Advanced techniques in echocardiography in small animals. Vet Clin North Am Small Anim Pract. 2010;40:529–543.
182. Chetboul V, Athanassiadis N, Carlos Sampedrano C, et al. Quantification, repeatability, and reproducibility of feline radial and longitudinal left ventricular velocities by tissue Doppler imaging. Am J Vet Res. 2004;65:566–572.
183. Wess G, Sarkar R, Hartmann K. Assessment of left ventricular systolic function by strain imaging echocardiography in various stages of feline hypertrophic cardiomyopathy. J Vet Intern Med. 2010;24:1375–1382.
184. Rajagopalan N, Garcia M.J, Rodriguez L, et al. Comparison of new Doppler echocardiographic methods to differentiate constrictive pericardial heart disease and restrictive cardiomyopathy. Am J Cardiol. 2001;87:86–94.
185. MacDonald K.A, Wisner E.R, Larson R.F, et al. Comparison of myocardial contrast enhancement via cardiac magnetic resonance imaging in healthy cats and cats with hypertrophic cardiomyopathy. Am J Vet Res. 2005;66:1891–1894.
186. MacDonald K.A, Kittleson M.D, Garcia-Nolen T, et al. Tissue Doppler imaging and gradient echo cardiac magnetic resonance imaging in normal cats and cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2006;20:627–634.
187. MacDonald K.A, Kittleson M.D, Larson R.F, et al. The effect of ramipril on left ventricular mass, myocardial fibrosis, diastolic function, and plasma neurohormones in Maine Coon cats with familial hypertrophic cardiomyopathy without heart failure. J Vet Intern Med. 2006;20:1093–1105.
188. Romito G, Guglielmini C, Mazzarella M.O, et al. Diagnostic and prognostic utility of surface electrocardiography in cats with left ventricular hypertrophy. J Vet Cardiol. 2018;20:364–375.
189. Langhorn R, Tarnow I, Willesen J.L, et al. Cardiac troponin I and T as prognostic markers in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2014;28:1485–1491.
190. Borgeat K, Sherwood K, Payne J.R, et al. Plasma cardiac troponin I concentration and cardiac death in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2014;28:1731–1737.
191. Hori Y, Iguchi M, Heishima Y, et al. Diagnostic utility of cardiac troponin I in cats with hypertrophic cardiomyopathy. J Vet Intern Med. 2018;32:922–929.
192. Hertzsch S, Roos A, Wess G. Evaluation of a sensitive cardiac troponin I assay as a screening test for the diagnosis of hypertrophic cardiomyopathy in cats. J Vet Intern Med. 2019;33:1242–1250.
193. Wess G, Daisenberger P, Mahling M, et al. Utility of measuring plasma N-terminal pro-brain natriuretic peptide in detecting hypertrophic cardiomyopathy and differentiating grades of severity in cats. Vet Clin Pathol. 2011;40:237–244.
194. Oyama M.A, Boswood A, Connolly D.J, et al. Clinical usefulness of an assay for measurement of circulating N-terminal pro-B-type natriuretic peptide concentration in dogs and cats with heart disease. J Am Vet Med Assoc. 2013;243:71–82.
195. Singletary G.E, Rush J.E, Fox P.R, et al. Effect of NT-pro-BNP assay on accuracy and confidence of general practitioners in diagnosing heart failure or respiratory disease in cats with respiratory signs. J Vet Intern Med. 2012;26:542–546.
196. Fox P.R, Oyama M.A, Reynolds C, et al. Utility of plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) to distinguish between congestive heart failure and non-cardiac causes of acute dyspnea in cats. J Vet Cardiol. 2009;11:S51–S61.
197. Hezzell M.J, Rush J.E, Humm K, et al. Differentiation of cardiac from noncardiac pleural effusions in cats using second-generation quantitative and point-of-care NT-proBNP measurements. J Vet Intern Med. 2016;30:536–542.
198. Wurtinger G, Henrich E, Hildebrandt N, et al. Assessment of a bedside test for N-terminal pro B-type natriuretic peptide (NT-proBNP) to differentiate cardiac from non-cardiac causes of pleural effusion in cats. BMC Vet Res. 2017;13:394.
199. Fox P.R, Rush J.E, Reynolds C.A, et al. Multicenter evaluation of plasma N-terminal probrain natriuretic peptide (NT-pro BNP) as a biochemical screening test for asymptomatic (occult) cardiomyopathy in cats. J Vet Intern Med. 2011;25:1010–1016.
200. Machen M.C, Oyama M.A, Gordon S.G, et al. Multi-centered investigation of a point-of-care NT-proBNP ELISA assay to detect moderate to severe occult (pre-clinical) feline heart disease in cats referred for cardiac evaluation. J Vet Cardiol. 2014;16:245–255.
201. Harris A.N, Beatty S.S, Estrada A.H, et al. Investigation of an N-terminal prohormone of brain natriuretic peptide point-of-care ELISA in clinically normal cats and cats with cardiac disease. J Vet Intern Med. 2017;31:994–999.
202. Ljungvall I, Rishniw M, Porciello F, et al. Sleeping and resting respiratory rates in healthy adult cats and cats with subclinical heart disease. J Feline Med Surg. 2014;16:281–290.
203. Maron B.J, McKenna W.J, Danielson G.K, et al. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687–1713.
204. Hogan D.F, Fox P.R, Jacob K, et al. Secondary prevention of cardiogenic arterial thromboembolism in the cat: the double-blind, randomized, positive-controlled feline arterial thromboembolism; clopidogrel vs. aspirin trial (FAT CAT). J Vet Cardiol. 2015;17:S306–S317.
205. Dixon-Jimenez A.C, Brainard B.M, Brooks M.B, et al. Pharmacokinetic and pharmacodynamic evaluation of oral rivaroxaban in healthy adult cats. J Vet Emerg Crit Care (San Antonio). 2016;26:619–629.
206. Lo S.T, Walker A.L, Georges C.J, et al. Dual therapy with clopidogrel and rivaroxaban in cats with thromboembolic disease. J Feline Med Surg. 2022;24:277–283.
207. Sharp C.R, deLaforcade A.M, Koenigshof A.M, et al. Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE): Domain 4-Refining and monitoring antithrombotic therapies. J Vet Emerg Crit Care (San Antonio). 2019;29:75–87.
208. Cherian G, Brockington I.F, Shah P.M, et al. Beta-adrenergic blockade in hypertrophic obstructive cardiomyopathy. Br Med J. 1966;1:895–898.
209. Coleman A.E, DeFrancesco T.C, Griffiths E.H, et al. Atenolol in cats with subclinical hypertrophic cardiomyopathy: a double-blind, placebo-controlled, randomized clinical trial of effect on quality of life, activity, and cardiac biomarkers. J Vet Cardiol. 2020;30:77–91.
210. Jung S.W, Kittleson M.D. The effect of atenolol on NT-proBNP and troponin in asymptomatic cats with severe left ventricular hypertrophy because of hypertrophic cardiomyopathy: a pilot study. J Vet Intern Med. 2011;25:1044–1049.
211. Riesen S.C, Schober K.E, Cervenec R.M, et al. Comparison of the effects of ivabradine and atenolol on heart rate and echocardiographic variables of left heart function in healthy cats. J Vet Intern Med. 2011;25:469–476.
212. Betocchi S, Piscione F, Losi M.A, et al. Effects of diltiazem on left ventricular systolic and diastolic function in hypertrophic cardiomyopathy. Am J Cardiol. 1996;78:451–457.
213. Bright J.M, Golden A.L, Gompf R.E, et al. Evaluation of the calcium channel-blocking agents diltiazem and verapamil for treatment of feline hypertrophic cardiomyopathy. J Vet Intern Med. 1991;5:272–282.
214. Sadoshima J, Izumo S. Molecular characterization of angiotensin II-induced hypertrophy of cardiac myocytes and hyperplasia of cardiac fibroblasts. Critical role of the AT1 receptor subtype. Circ Res. 1993;73:413–423.
215. Brilla C.G, Matsubara L.S, Weber K.T. Antifibrotic effects of spironolactone in preventing myocardial fibrosis in systemic arterial hypertension. Am J Cardiol. 1993;71:12A–A.
216. Tsybouleva N, Zhang L, Chen S, et al. Aldosterone, through novel signaling proteins, is a fundamental molecular bridge between the genetic defect and the cardiac phenotype of hypertrophic cardiomyopathy. Circulation. 2004;109:1284–1291.
217. Lim D.S, Lutucuta S, Bachireddy P, et al. Angiotensin II blockade reverses myocardial fibrosis in a transgenic mouse model of human hypertrophic cardiomyopathy. Circulation. 2001;103:7897–7891.
218. Zhong J, Basu R, Guo D, et al. Angiotensin-converting enzyme 2 suppresses pathological hypertrophy, myocardial fibrosis, and cardiac dysfunction. Circulation. 2010;122:717–728.
219. de Resende M.M, Kriegel A.J, Greene A.S. Combined effects of low-dose spironolactone and captopril therapy in a rat model of genetic hypertrophic cardiomyopathy. J Cardiovasc Pharmacol. 2006;48:265–273.
220. Taillefer M, Di Fruscia R. Benazepril and subclinical feline hypertrophic cardiomyopathy: a prospective, blinded, controlled study. Can Vet J. 2006;47:437–445.
221. MacDonald K.A, Kittleson M.D, Kass P.H, et al. Effect of spironolactone on diastolic function and left ventricular mass in Maine Coon cats with familial hypertrophic cardiomyopathy. J Vet Intern Med. 2008;22:335–341.
222. van Hoek I, Hodgkiss-Geere H, Bode E.F, et al. Association of diet with left ventricular wall thickness, troponin I and IGF-1 in cats with subclinical hypertrophic cardiomyopathy. J Vet Intern Med. 2020;34:2197–2210.
223. Uechi M, Matsuoka M, Kuwajima E, et al. The effects of the loop diuretics furosemide and torasemide on diuresis in dogs and cats. J Vet Med Sci. 2003;65:1057–1061.
224. DeFrancesco T.C. Management of cardiac emergencies in small animals. Vet Clin North Am Small Anim Pract. 2013;43:817–842.
225. Ueda Y, Li R.H.L, Nguyen N, et al. A genetic polymorphism in P2RY(1) impacts response to clopidogrel in cats with hypertrophic cardiomyopathy. Sci Rep. 2021;11:12522.
226. Rush J.E, Freeman L.M, Brown D.J, et al. The use of enalapril in the treatment of feline hypertrophic cardiomyopathy. J Am Anim Hosp Assoc. 1998;34:38–41.
227. Amberger C.N, Glardon O, Glaus T, et al. Effects of benazepril in the treatment of feline hypertrophic cardiomyopathy Results of a prospective, open-label, multicenter clinical trial. J Vet Cardiol. 1999;1:19–26.
228. Fox P.R. Prospective, double-blinded, multicenter evaluation of chronic therapies for feline diastolic heart failure: interim analysis. The Multicenter Feline Chronic Heart Failure Study Group. In: Proceedings. 21st American College of Veterinary Internal Medicine Forum. Charlotte; 2003:398–399.
229. King J.N, Martin M, Chetboul V, et al. Evaluation of benazepril in cats with heart disease in a prospective, randomized, blinded, placebo-controlled clinical trial. J Vet Intern Med. 2019;33:2559–2571.
230. Hanzlicek A.S, Gehring R, KuKanich B. Pharmacokinetics of oral pimobendan in healthy cats. J Vet Cardiol. 2012;14:489–496.
231. Reina-Doreste Y, Stern J.A, Keene B.W, et al. Case-control study of the effects of pimobendan on survival time in cats with hypertrophic cardiomyopathy and congestive heart failure. J Am Vet Med Assoc. 2014;245:534–539.
232. Gordon S.G, Saunders A.B, Roland R.M, et al. Effect of oral administration of pimobendan in cats with heart failure. J Am Vet Med Assoc. 2012;241:89–94.
233. Macgregor J.M, Rush J.E, Laste N.J, et al. Use of pimobendan in 170 cats (2006-2010). J Vet Cardiol. 2011;13:251–260.
234. Oldach M.S, Ueda Y, Ontiveros E.S, et al. Cardiac effects of a single dose of pimobendan in cats with hypertrophic cardiomyopathy; a randomized, placebo-controlled, crossover study. Front Vet Sci. 2019;6:15.
235. Kochie S.L, Schober K.E, Rhinehart J, et al. Effects of pimobendan on left atrial transport function in cats. J Vet Intern Med. 2021;35:10–21.
236. Schober K.E, Rush J.E, Luis Fuentes V, et al. Effects of pimobendan in cats with hypertrophic cardiomyopathy and recent congestive heart failure: results of a prospective, double-blind, randomized, nonpivotal, exploratory field study. J Vet Intern Med. 2021;35:789–800.
237. Ward J.L, Kussin E.Z, Tropf M.A, et al. Retrospective evaluation of the safety and tolerability of pimobendan in cats with obstructive vs nonobstructive cardiomyopathy. J Vet Intern Med. 2020;34:2211–2222.
238. Poissonnier C, Ghazal S, Passavin P, et al. Tolerance of torasemide in cats with congestive heart failure: a retrospective study on 21 cases (2016-2019). BMC Vet Res. 2020;16:339.
239. James R, Guillot E, Garelli-Paar C, et al. The SEISICAT study: a pilot study assessing efficacy and safety of spironolactone in cats with congestive heart failure secondary to cardiomyopathy. J Vet Cardiol. 2018;20:1–12.
240. Atkins C.E, Snyder P.S, Keene B.W, et al. Efficacy of digoxin for treatment of cats with dilated cardiomyopathy. J Am Vet Med Assoc. 1990;196:1463–1469.